Center for Stroke Research Berlin, Charité - Universitätsmedizin Berlin, Charitéplatz 1, 10117 Berlin, Germany.
BMC Neurol. 2009 Dec 8;9:60. doi: 10.1186/1471-2377-9-60.
The mismatch between diffusion weighted imaging (DWI) lesion and perfusion imaging (PI) deficit volumes has been used as a surrogate of ischemic penumbra. This pathophysiology-orientated patient selection criterion for acute stroke treatment may have the potential to replace a fixed time window. Two recent trials - DEFUSE and EPITHET - investigated the mismatch concept in a multicenter prospective approach. Both studies randomized highly selected patients (n = 74/n = 100) and therefore confirmation in a large consecutive cohort is desirable. We here present a single-center approach with a 3T MR tomograph next door to the stroke unit, serving as a bridge from the ER to the stroke unit to screen all TIA and stroke patients. Our primary hypothesis is that the prognostic value of the mismatch concept is depending on the vessel status. Primary endpoint of the study is infarct growth determined by imaging, secondary endpoints are neurological deficit on day 5-7 and functional outcome after 3 months.
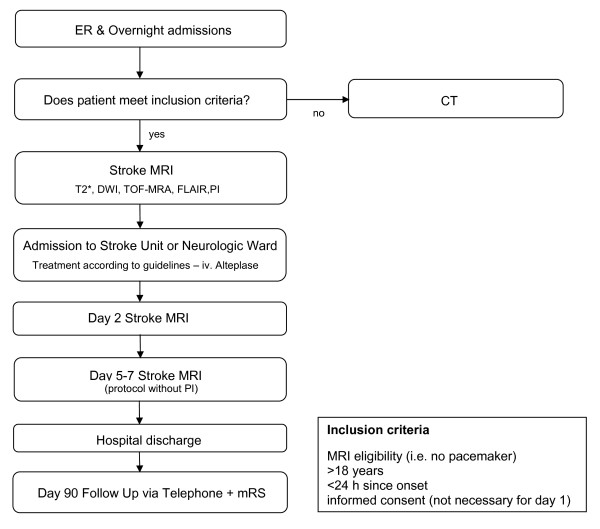
1000Plus is a prospective, single centre observational study with 1200 patients to be recruited. All patients admitted to the ER with the clinical diagnosis of an acute cerebrovascular event within 24 hours after symptom onset are screened. Examinations are performed on day 1, 2 and 5-7 with neurological examination including National Institute of Health Stroke Scale (NIHSS) scoring and stroke MRI including T2*, DWI, TOF-MRA, FLAIR and PI. PI is conducted as dynamic susceptibility-enhanced contrast imaging with a fixed dosage of 5 ml 1 M Gadobutrol. For post-processing of PI, mean transit time (MTT) parametric images are determined by deconvolution of the arterial input function (AIF) which is automatically identified. Lesion volumes and mismatch are measured and calculated by using the perfusion mismatch analyzer (PMA) software from ASIST-Japan. Primary endpoint is the change of infarct size between baseline examination and day 5-7 follow up.
The aim of this study is to describe the incidence of mismatch and the predictive value of PI for final lesion size and functional outcome depending on delay of imaging and vascular recanalization. It is crucial to standardize PI for future randomized clinical trials as for individual therapeutic decisions and we expect to contribute to this challenging task.
clinicaltrials.gov NCT00715533.
弥散加权成像(DWI)病变与灌注成像(PI)缺损体积之间的不匹配已被用作缺血半暗带的替代指标。这种基于病理生理学的急性卒中治疗患者选择标准可能具有取代固定时间窗的潜力。两项最近的试验——DEFUSE 和 EPITHET——以多中心前瞻性方法研究了不匹配的概念。这两项研究均对高度选择的患者(n = 74/n = 100)进行了随机分组,因此在大型连续队列中进行确认是理想的。我们在此介绍了一种单中心方法,该方法使用隔壁的 3T 磁共振断层扫描仪作为从急诊室到卒中单元的桥梁,以筛查所有 TIA 和卒中患者。我们的主要假设是不匹配概念的预后价值取决于血管状态。该研究的主要终点是通过影像学确定的梗死进展,次要终点是第 5-7 天的神经功能缺损和 3 个月后的功能结局。
1000Plus 是一项前瞻性、单中心观察性研究,预计将招募 1200 名患者。所有在症状发作后 24 小时内以急性脑血管事件的临床诊断被收入急诊室的患者均进行筛查。检查在第 1、2 天以及第 5-7 天进行,包括神经检查,包括国立卫生研究院卒中量表(NIHSS)评分和卒中 MRI,包括 T2*、DWI、TOF-MRA、FLAIR 和 PI。PI 是通过对自动识别的动脉输入函数(AIF)进行去卷积来进行动态对比增强磁共振成像。用于 PI 的后处理,通过使用来自 ASIST-Japan 的灌注不匹配分析器(PMA)软件来确定平均通过时间(MTT)参数图像。病变体积和不匹配通过灌注不匹配分析器(PMA)软件进行测量和计算。主要终点是基线检查与第 5-7 天随访之间的梗死面积变化。
本研究的目的是描述不匹配的发生率以及 PI 对最终病变大小和功能结局的预测价值,取决于成像延迟和血管再通。为了未来的随机临床试验和个体化治疗决策,对 PI 进行标准化是至关重要的,我们希望为这一具有挑战性的任务做出贡献。
clinicaltrials.gov NCT00715533。