Section for Biomedical Physics, University Hospital for Radiation Oncology, Hoppe-Seyler-Str, 3, 72076 Tübingen, Germany.
Radiat Oncol. 2009 Dec 12;4:64. doi: 10.1186/1748-717X-4-64.
The purpose of the present study is to compare finite size pencil beam (fsPB) and Monte Carlo (MC) based optimization of lung intensity-modulated stereotactic radiotherapy (lung IMSRT).
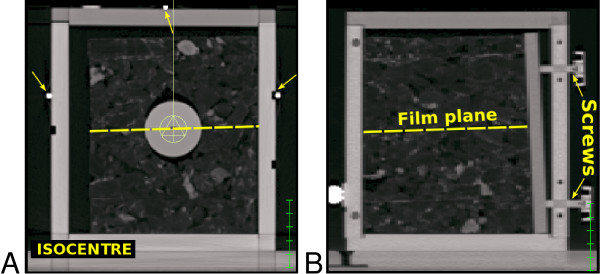
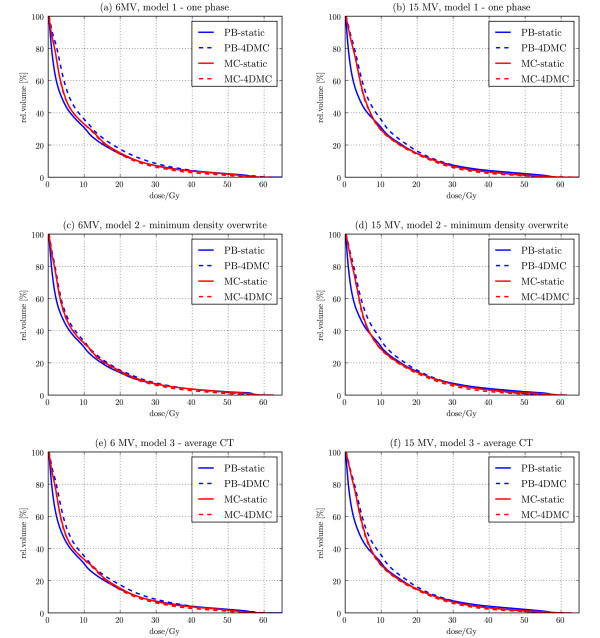
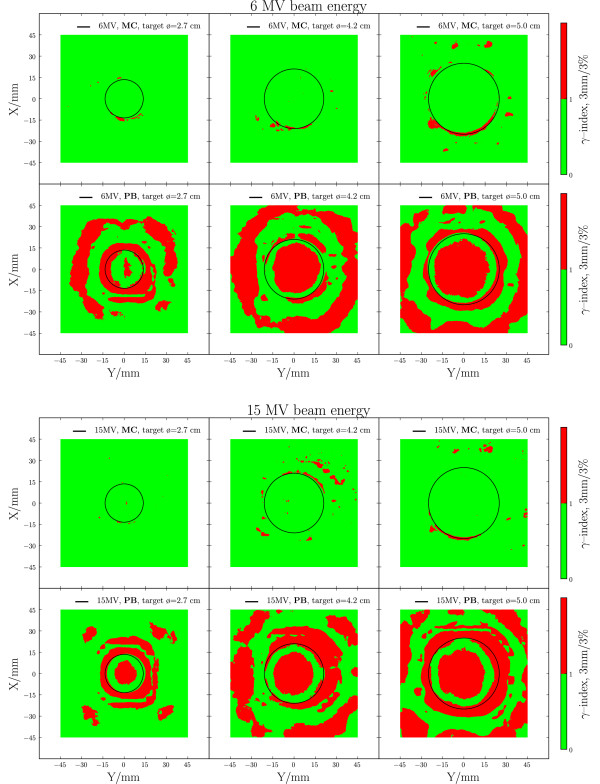
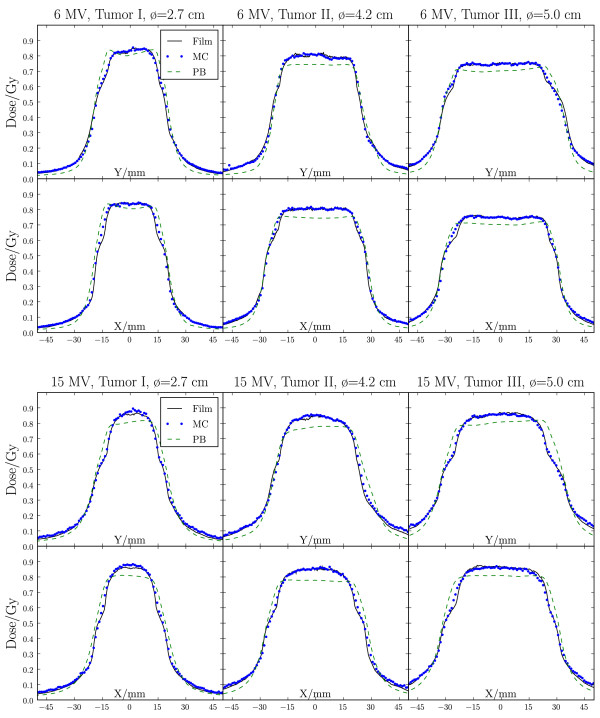
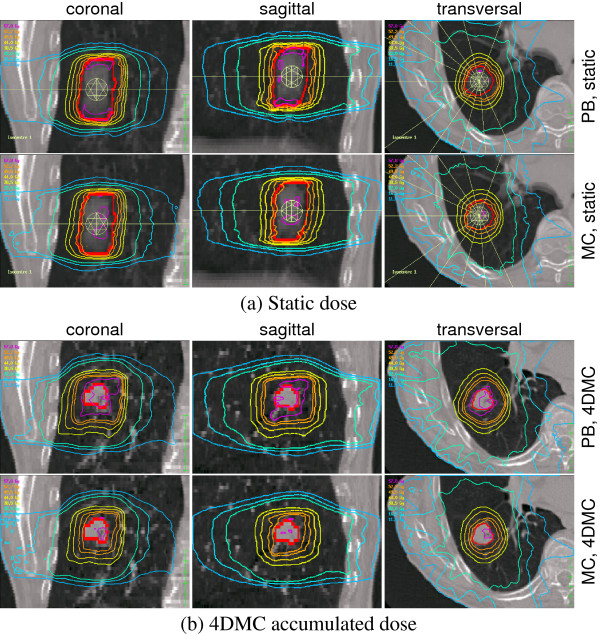
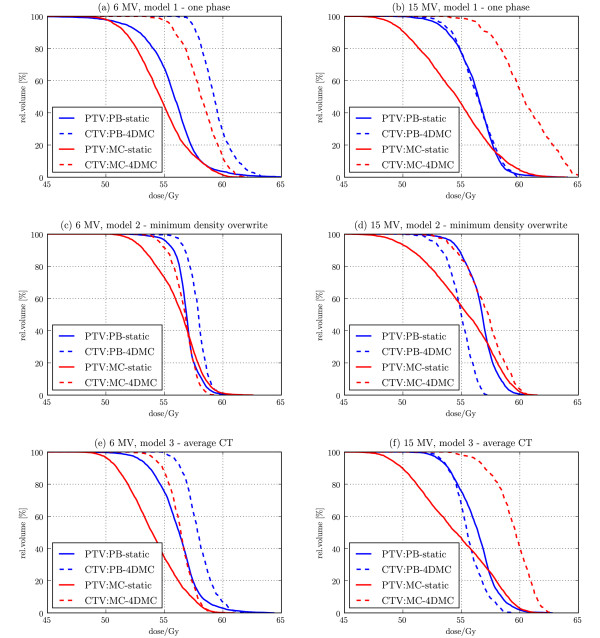
A fsPB and a MC algorithm as implemented in a biological IMRT planning system were validated by film measurements in a static lung phantom. Then, they were applied for static lung IMSRT planning based on three different geometrical patient models (one phase static CT, density overwrite one phase static CT, average CT) of the same patient. Both 6 and 15 MV beam energies were used. The resulting treatment plans were compared by how well they fulfilled the prescribed optimization constraints both for the dose distributions calculated on the static patient models and for the accumulated dose, recalculated with MC on each of 8 CTs of a 4DCT set.
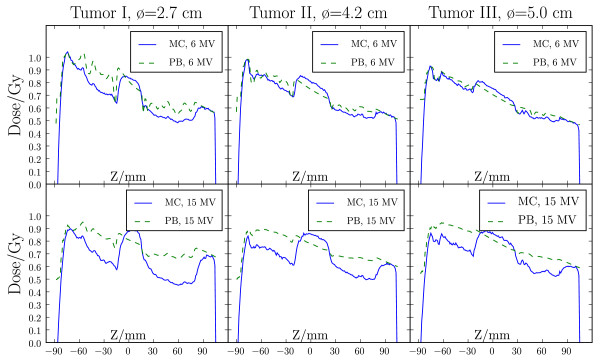
In the phantom measurements, the MC dose engine showed discrepancies < 2%, while the fsPB dose engine showed discrepancies of up to 8% in the presence of lateral electron disequilibrium in the target. In the patient plan optimization, this translates into violations of organ at risk constraints and unpredictable target doses for the fsPB optimized plans. For the 4D MC recalculated dose distribution, MC optimized plans always underestimate the target doses, but the organ at risk doses were comparable. The results depend on the static patient model, and the smallest discrepancy was found for the MC optimized plan on the density overwrite one phase static CT model.
It is feasible to employ the MC dose engine for optimization of lung IMSRT and the plans are superior to fsPB. Use of static patient models introduces a bias in the MC dose distribution compared to the 4D MC recalculated dose, but this bias is predictable and therefore MC based optimization on static patient models is considered safe.
本研究的目的是比较有限束笔形束(fsPB)和蒙特卡罗(MC)在肺部强度调制立体定向放射治疗(lung IMSRT)中的优化。
在静态肺部体模中使用胶片测量验证了一种生物 IMRT 计划系统中的 fsPB 和 MC 算法。然后,将它们应用于同一患者的三种不同几何患者模型(单相静态 CT、密度覆盖单相静态 CT、平均 CT)的静态肺部 IMSRT 计划。使用了 6 和 15 MV 两种射束能量。根据静态患者模型上计算的剂量分布和在 4DCT 集的 8 个 CT 上的每个 CT 上用 MC 重新计算的累积剂量,比较了治疗计划的结果。
在体模测量中,MC 剂量引擎的差异<2%,而在靶区存在横向电子失衡的情况下,fsPB 剂量引擎的差异高达 8%。在患者计划优化中,这转化为危及器官约束的违反和 fsPB 优化计划中不可预测的靶区剂量。对于 4D MC 重新计算的剂量分布,MC 优化计划总是低估靶区剂量,但危及器官剂量相当。结果取决于静态患者模型,MC 优化计划在密度覆盖单相静态 CT 模型上的差异最小。
可以使用 MC 剂量引擎对肺部 IMSRT 进行优化,并且计划优于 fsPB。使用静态患者模型会在 MC 剂量分布中引入与 4D MC 重新计算剂量相比的偏差,但这种偏差是可预测的,因此基于 MC 的静态患者模型优化被认为是安全的。