Department of Oncology and Radiotherapy, Turku University Hospital, POB 52, 20521 Turku, Finland.
Radiat Oncol. 2012 May 31;7:79. doi: 10.1186/1748-717X-7-79.
Stereotactic lung radiotherapy (SLRT) has emerged as a curative treatment for medically inoperable patients with early-stage non-small cell lung cancer (NSCLC) and the use of intensity-modulated radiotherapy (IMRT) and volumetric modulated arc treatments (VMAT) have been proposed as the best practical approaches for the delivery of SLRT. However, a large number of narrow field shapes are needed in the dose delivery of intensity-modulated techniques and the probability of underdosing the tumour periphery increases as the effective field size is decreased. The purpose of this study was to evaluate small lung tumour doses irradiated by intensity-modulated techniques to understand the risk for dose calculation errors in precision radiotherapy such as SLRT.
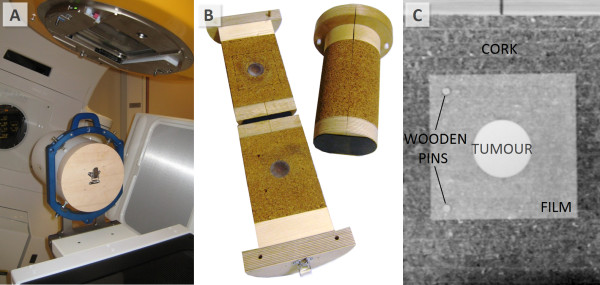
The study was executed with two heterogeneous phantoms with targets of Ø1.5 and Ø4.0 cm. Dose distributions in the simulated tumours delivered by small sliding window apertures (SWAs), IMRT and RapidArc treatment plans were measured with radiochromic film. Calculation algorithms of pencil beam convolution (PBC) and anisotropic analytic algorithm (AAA) were used to calculate the corresponding dose distributions.
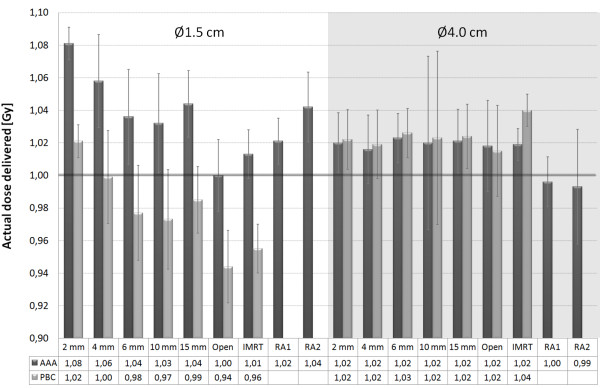
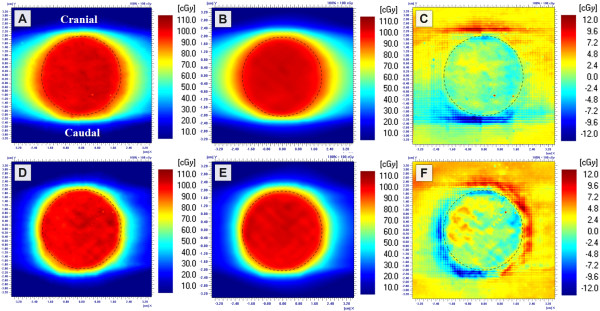
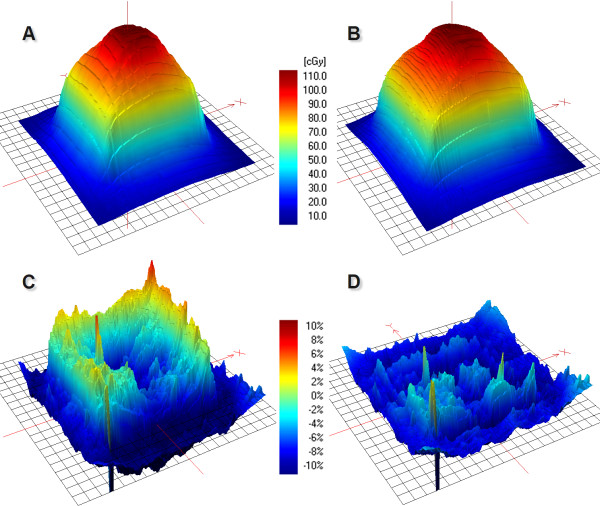
Peripheral doses of the tumours were decreased as SWA decreased, which was not modelled by the calculation algorithms. The smallest SWA studied was 2 mm, which reduced the 90% isodose line width by 4.2 mm with the Ø4.0 cm tumour as compared to open field irradiation. PBC was not able to predict the dose accurately as the gamma evaluation failed to meet the criteria of ±3%/±1 mm on average in 61% of the defined volume with the smaller tumour. With AAA the corresponding value was 16%. The dosimetric inaccuracy of AAA was within ±3% with the optimized treatment plans of IMRT and RapidArc. The exception was the clinical RapidArc plan with dose overestimation of 4%.
Overall, the peripheral doses of the simulated lung tumours were decreased by decreasing the SWA. To achieve adequate surface dose coverage to small lung tumours with a difference less than 1 mm in the isodose line radius between the open and modulated field, a larger than 6 mm SWA should be used in the dose delivery of SLRT.
立体定向肺部放疗(SLRT)已成为不能手术的早期非小细胞肺癌(NSCLC)患者的一种有治愈可能的治疗方法,调强放疗(IMRT)和容积旋转调强治疗(VMAT)的应用被认为是实现 SLRT 剂量传递的最佳实用方法。然而,在调强技术的剂量传递中需要大量的窄野形状,并且随着有效野尺寸的减小,肿瘤边缘的欠剂量概率增加。本研究的目的是评估强度调制技术照射的小肺肿瘤剂量,以了解 SLRT 等精准放疗中剂量计算误差的风险。
本研究使用两个异质体模进行,靶标为 Ø1.5 和 Ø4.0cm。通过放射色胶片测量模拟肿瘤中由小滑动窗口孔径(SWA)、调强放疗和 RapidArc 治疗计划输送的剂量分布。使用铅笔束卷积(PBC)和各向异性解析算法(AAA)计算算法计算相应的剂量分布。
随着 SWA 的减小,肿瘤的外周剂量降低,而这并未被计算算法所模拟。研究中最小的 SWA 为 2mm,与开放野照射相比,Ø4.0cm 肿瘤的 90%等剂量线宽度减小了 4.2mm。由于伽玛评估在 61%的定义体积中平均未能满足±3%/±1mm 的标准,PBC 无法准确预测剂量,而对于较小的肿瘤,该值为 16%。AAA 的剂量学误差在±3%以内,适用于优化的 IMRT 和 RapidArc 治疗计划。例外的是临床 RapidArc 计划,剂量高估了 4%。
总的来说,随着 SWA 的减小,模拟肺肿瘤的外周剂量降低。为了在开放和调制野之间等剂量线半径相差小于 1mm 的情况下为小肺肿瘤提供足够的表面剂量覆盖,SLRT 剂量传递中应使用大于 6mm 的 SWA。