Australian Centre for Economic Research on Health, The Australian National University, Canberra ACT 0200, Australia.
BMC Public Health. 2009 Dec 14;9:460. doi: 10.1186/1471-2458-9-460.
In Australia there is a socioeconomic gradient in morbidity and mortality favouring socioeconomically advantaged people, much of which is accounted for by ischaemic heart disease. This study examines if Australia's universal health care system, with its mixed public/private funding and delivery model, may actually perpetuate this inequity. We do this by quantifying and comparing socioeconomic inequalities in the receipt of coronary procedures in patients with acute myocardial infarction (AMI) and patients with angina.
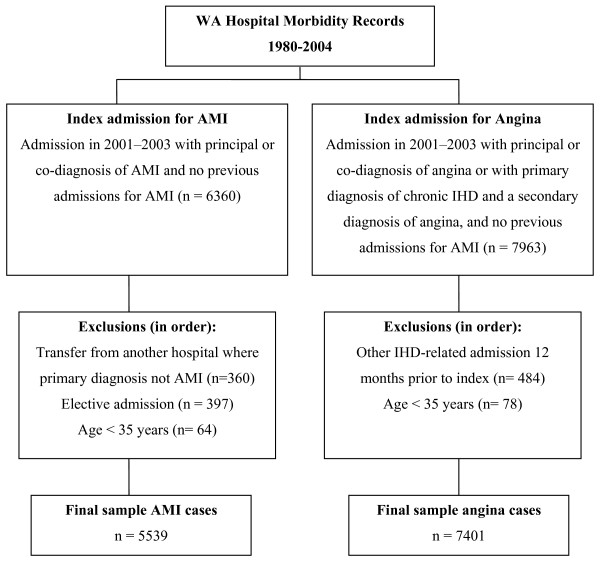
Using linked hospital and mortality data, we followed patients admitted to Western Australian hospitals with a first admission for AMI (n = 5539) or angina (n = 7401) in 2001-2003. An outcome event was the receipt, within a year, of a coronary procedure-angiography, angioplasty and/or coronary artery bypass surgery (CABG). Socioeconomic status was assigned to each individual using an area-based measure, the SEIFA Index of Disadvantage. Multivariable proportional hazards regression was used to model the association between socioeconomic status and procedure rates, allowing for censoring and adjustment of multiple covariates. Mediating models examined the effect of private health insurance.
In the AMI patient cohort, socioeconomic gradients were not evident except that disadvantaged women were more likely than advantaged women to undergo CABG. In contrast, in the angina patient group there were clear socioeconomic gradients for all procedures, favouring more advantaged patients. Compared with patients in the most disadvantaged quintile of socioeconomic status, patients in the least disadvantaged quintile were 11% (1-21%) more likely to receive angiography, 52% (29-80%) more likely to undergo angioplasty and 30% (3-55%) more likely to undergo CABG. Private health insurance explained some of the socioeconomic variation in rates.
Australia's universal health care system does not guarantee equity in the receipt of high technology health care for patients with ischaemic heart disease. While such a system might ensure equity for patients with AMI, where guidelines for treatment are relatively well established, this is not the case for angina patients, where health care may be less urgent and more discretionary.
在澳大利亚,发病率和死亡率存在社会经济梯度,有利于社会经济地位较高的人群,其中大部分归因于缺血性心脏病。本研究通过量化和比较急性心肌梗死(AMI)和心绞痛患者接受冠状动脉介入治疗的社会经济不平等,探讨澳大利亚的全民医疗保健系统(其混合公共/私人筹资和提供模式)是否会加剧这种不平等。我们使用链接的医院和死亡率数据,对 2001-2003 年在西澳大利亚医院首次因 AMI(n=5539)或心绞痛(n=7401)住院的患者进行了随访。主要结局是在一年内接受冠状动脉介入治疗-血管造影、经皮冠状动脉成形术和/或冠状动脉旁路移植术(CABG)。使用基于区域的指标,即社会经济地位劣势指数(SEIFA 指数),为每位个体分配社会经济地位。多变量比例风险回归用于模拟社会经济地位与手术率之间的关系,允许进行删失和对多个协变量进行调整。中介模型检验了私人医疗保险的影响。
在 AMI 患者队列中,除了处于不利地位的女性比处于有利地位的女性更有可能接受 CABG 外,没有明显的社会经济梯度。相比之下,在心绞痛患者组中,所有手术都存在明显的社会经济梯度,有利于更有利的患者。与社会经济地位最不利五分位数的患者相比,最有利五分位数的患者接受血管造影的可能性高 11%(1-21%),接受经皮冠状动脉成形术的可能性高 52%(29-80%),接受 CABG 的可能性高 30%(3-55%)。私人医疗保险解释了部分社会经济差异的原因。
澳大利亚的全民医疗保健系统并不能保证缺血性心脏病患者接受高科技医疗保健的公平性。虽然这种系统可能确保了 AMI 患者的公平性,因为治疗指南相对明确,但对于心绞痛患者则不然,因为他们的医疗保健可能不那么紧急,更具选择性。