Paulden Mike, Palmer Stephen, Hewitt Catherine, Gilbody Simon
Centre for Health Economics, University of York, Heslington, York YO10 5DD.
BMJ. 2009 Dec 22;339:b5203. doi: 10.1136/bmj.b5203.
To evaluate the cost effectiveness of routine screening for postnatal depression in primary care.
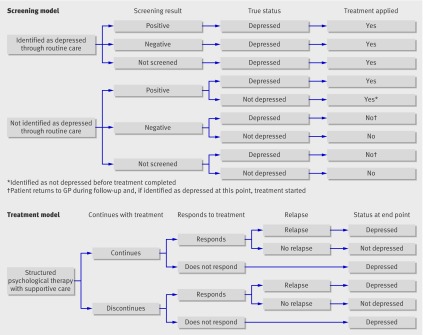
Cost effectiveness analysis with a decision model of alternative methods of screening for depression, including standardised postnatal depression and generic depression instruments. The performance of screening instruments was derived from a systematic review and bivariate meta-analysis at a range of instrument cut points; estimates of other relevant parameters were derived from literature sources and relevant databases. A decision tree considered the full treatment pathway from the possible onset of postnatal depression through identification, treatment, and possible relapse.
Primary care.
A hypothetical population of women assessed for postnatal depression either via routine care only or supplemented by use of formal identification methods six weeks postnatally, as recommended in recent guidelines.
Costs expressed in 2006-7 prices and impact on health outcomes expressed in terms of quality adjusted life years (QALYs). The time horizon of the analysis was one year.
The routine application of either postnatal or general depression questionnaires did not seem to be cost effective compared with routine care only. The Edinburgh postnatal depression scale (at a cut point of 16) had an incremental cost effectiveness ratio (ICER) of pound 41,103 (euro 45,398, $67,130) per QALY compared with routine care only. The ICER for all other strategies ranged from pound 49,928 to pound 272,463 per QALY versus routine care only, while the probability that no formal identification strategy was cost effective was 88% (59%) at a cost effectiveness threshold of pound 20,000 ( pound 30,000) per QALY. While sensitivity analysis indicated that the cost of managing incorrectly identified depression (false positive result) was an important driver of the model, formal identification approaches did not seem to be cost effective at any feasible estimate of this cost.
Formal identification methods for postnatal depression do not seem to represent value for money for the NHS. The major determinant of cost effectiveness seems to be the potential additional costs of managing women incorrectly diagnosed as depressed. Formal identification methods for postnatal depression do not currently satisfy the National Screening Committee's criteria for the adoption of a screening strategy as part of national health policy.
评估初级保健中产后抑郁症常规筛查的成本效益。
采用成本效益分析,构建抑郁症筛查替代方法的决策模型,包括标准化产后抑郁量表和通用抑郁量表。筛查工具的性能源自系统评价和在一系列工具切点处的双变量荟萃分析;其他相关参数的估计值来自文献资料和相关数据库。决策树考虑了从产后抑郁症可能发病开始,经过识别、治疗以及可能复发的完整治疗路径。
初级保健。
假设的女性群体,她们要么仅通过常规护理接受产后抑郁症评估,要么按照近期指南的建议,在产后六周通过使用正式识别方法进行补充评估。
以2006 - 2007年价格表示的成本,以及以质量调整生命年(QALYs)表示的对健康结局的影响。分析的时间范围为一年。
与仅进行常规护理相比,常规应用产后或通用抑郁问卷似乎不具有成本效益。与仅进行常规护理相比,爱丁堡产后抑郁量表(切点为16)每获得一个QALY的增量成本效益比(ICER)为41,103英镑(45,398欧元,67,130美元)。与仅进行常规护理相比,所有其他策略的ICER范围为每QALY 49,928英镑至272,463英镑,而在每QALY成本效益阈值为20,000英镑(30,000英镑)时,没有正式识别策略具有成本效益的概率为88%(59%)。虽然敏感性分析表明,管理错误识别的抑郁症(假阳性结果)的成本是该模型的一个重要驱动因素,但在对该成本的任何可行估计下,正式识别方法似乎都不具有成本效益。
产后抑郁症的正式识别方法对英国国民医疗服务体系(NHS)而言似乎并不物有所值。成本效益的主要决定因素似乎是管理被错误诊断为抑郁症的女性的潜在额外成本。产后抑郁症的正式识别方法目前不符合国家筛查委员会作为国家卫生政策一部分采用筛查策略的标准。