Sunnybrook Health Sciences Center, 2075 Bayview Avenue, Toronto, Ontario, Canada.
BMC Health Serv Res. 2010 Jan 5;10:5. doi: 10.1186/1472-6963-10-5.
Despite universal health care, there continues to be regional access disparities to coronary angiography in Canada. Our objective was to evaluate the extent to which demand-side factors such as clinical urgency/need, and supply-side factors, as reflected by differences in physician and procedural supply account for these inequalities.
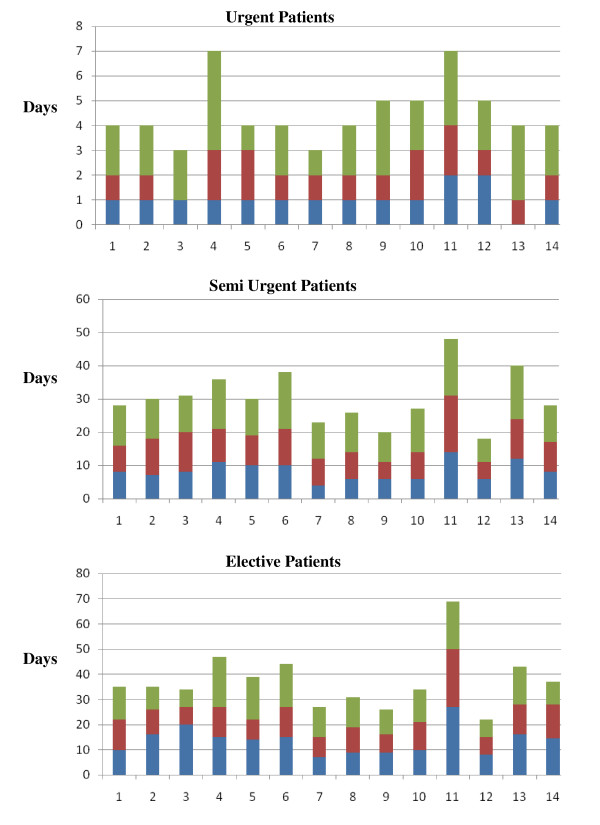
Our cohort consisted of 74,254 consecutive patients referred for coronary angiography in Ontario, Canada between April 1st 2005 and March 31st 2006, divided into three urgency strata based on a clinical urgency scale. Cox-proportional hazard models were developed, adjusting for age, gender, socioeconomic status (SES), region, and urgency score, with greater hazard ratios (HR) indicating shorter wait times. To evaluate mediators of any residual wait-time differences, we examined the influence of the regional supply of cath lab facilities, invasive cardiologists and general practitioners (GP).
We found that the urgency score was a significant predictor of wait time in all three strata (urgent patients: HR 1.61 for each unit increase in patient urgency (95% Confidence interval (CI) 1.55-1.67); semi-urgent patients: HR 1.55 (95% CI 1.44-1.68); elective patients: HR 1.13 (95% CI 1.08-1.18)). After accounting for clinical need/urgency, regional wait time differences persisted; these were most consistently associated with variation in cath lab supply. The impact of invasive cardiologist supply was restricted to urgent patients while that of GP supply was confined to semi-urgent and elective patients.
We found that there remained significant regional disparities in access to coronary angiography after accounting for clinical need. These disparities are partially explained by variations in supply of both procedural capacity and physician services, most notably in elective and semi-urgent patients.
尽管加拿大实行全民医保,但在接受冠状动脉造影检查方面仍存在地区差异。我们的目的是评估需求侧因素(如临床紧急/需求)和供给侧因素(如医生和手术供应的差异)在多大程度上解释了这些不平等现象。
我们的队列包括 2005 年 4 月 1 日至 2006 年 3 月 31 日期间在加拿大安大略省接受冠状动脉造影检查的 74254 例连续患者,根据临床紧急程度量表分为三个紧急程度层次。采用 Cox 比例风险模型进行分析,调整了年龄、性别、社会经济状况(SES)、地区和紧急程度评分,风险比(HR)越大表示等待时间越短。为了评估任何剩余等待时间差异的中介因素,我们检查了区域 cath 实验室设施、介入心脏病专家和全科医生(GP)供应的影响。
我们发现,在所有三个层次上,紧急程度评分都是等待时间的重要预测因素(紧急患者:每增加一个单位的患者紧急程度,HR 为 1.61(95%置信区间(CI)为 1.55-1.67);半紧急患者:HR 为 1.55(95% CI 为 1.44-1.68);择期患者:HR 为 1.13(95% CI 为 1.08-1.18))。在考虑到临床需求/紧急情况后,区域等待时间差异仍然存在;这些差异与 cath 实验室供应的变化最为一致。介入心脏病专家供应的影响仅限于紧急患者,而全科医生供应的影响仅限于半紧急和择期患者。
我们发现,在考虑到临床需求后,接受冠状动脉造影检查的机会仍存在显著的地区差异。这些差异部分可以通过手术能力和医生服务的供应变化来解释,尤其是在择期和半紧急患者中。