University Clinic of Anesthesia, Innsbruck Medical University, Anichstr 35, A-6020 Innsbruck, Austria.
Biomed Eng Online. 2010 Jan 6;9:2. doi: 10.1186/1475-925X-9-2.
Interruption of cardiopulmonary resuscitation (CPR) impairs the perfusion of the fibrillating heart, worsening the chance for successful defibrillation. Therefore ECG-analysis during ongoing chest compression could provide a considerable progress in comparison with standard analysis techniques working only during "hands-off" intervals.
For the reduction of CPR-related artifacts in ventricular fibrillation ECG we use a localized version of the coherent line removal algorithm developed by Sintes and Schutz. This method can be used for removal of periodic signals with sufficiently coupled harmonics, and can be adapted to specific situations by optimal choice of its parameters (e.g., the number of harmonics considered for analysis and reconstruction). Our testing was done with 14 different human ventricular fibrillation (VF) ECGs, whose fibrillation band lies in a frequency range of [1 Hz, 5 Hz]. The VF-ECGs were mixed with 12 different ECG-CPR-artifacts recorded in an animal experiment during asystole. The length of each of the ECG-data was chosen to be 20 sec, and testing was done for all 168 = 14 x 12 pairs of data. VF-to-CPR ratio was chosen as -20 dB, -15 dB, -10 dB, -5 dB, 0 dB, 5 dB and 10 dB. Here -20 dB corresponds to the highest level of CPR-artifacts.
For non-optimized coherent line removal based on signals with a VF-to-CPR ratio of -20 dB, -15 dB, -10 dB, -5 dB and 0 dB, the signal-to-noise gains (SNR-gains) were 9.3 +/- 2.4 dB, 9.4 +/- 2.4 dB, 9.5 +/- 2.5 dB, 9.3 +/- 2.5 dB and 8.0 +/- 2.7 (mean +/- std, n = 168), respectively. Characteristically, an original VF-to-CPR ratio of -10 dB, corresponds to a variance ratio var(VF):var(CPR) = 1:10. An improvement by 9.5 dB results in a restored VF-to-CPR ratio of -0.5 dB, corresponding to a variance ratio var(VF):var(CPR) = 1:1.1, the variance of the CPR in the signal being reduced by a factor of 8.9.
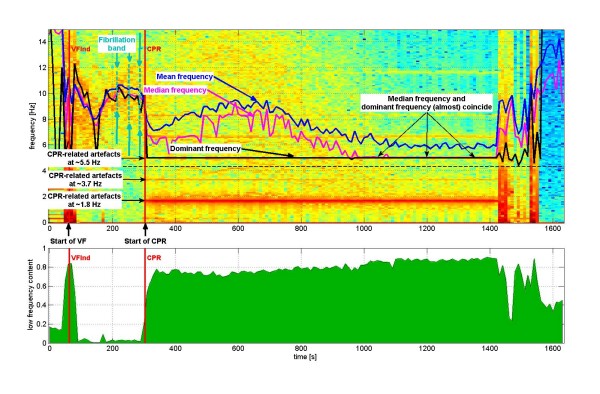
The localized coherent line removal algorithm uses the information of a single ECG channel. In contrast to multi-channel algorithms, no additional information such as thorax impedance, blood pressure, or pressure exerted on the sternum during CPR is required. Predictors of defibrillation success such as mean and median frequency of VF-ECGs containing CPR-artifacts are prone to being governed by the harmonics of the artifacts. Reduction of CPR-artifacts is therefore necessary for determining reliable values for estimators of defibrillation success.
The localized coherent line removal algorithm reduces CPR-artifacts in VF-ECG, but does not eliminate them. Our SNR-improvements are in the same range as offered by multichannel methods of Rheinberger et al., Husoy et al. and Aase et al. The latter two authors dealt with different ventricular rhythms (VF and VT), whereas here we dealt with VF, only. Additional developments are necessary before the algorithm can be tested in real CPR situations.

心肺复苏(CPR)过程中中断会影响颤动心脏的灌注,降低除颤成功的机会。因此,与仅在“脱手”间隔期间工作的标准分析技术相比,在持续进行胸部按压过程中进行心电图分析可以提供相当大的进展。
为了减少室颤 ECG 中的 CPR 相关伪影,我们使用 Sintes 和 Schutz 开发的局部相干线去除算法。该方法可用于去除具有足够耦合谐波的周期性信号,并可通过最佳选择其参数(例如,考虑分析和重建的谐波数量)来适应特定情况。我们的测试是使用 14 个不同的人类室颤(VF)ECG 进行的,其颤动带位于 [1 Hz,5 Hz] 的频率范围内。VF-ECG 与在动物实验中停搏期间记录的 12 种不同的 ECG-CPR 伪影混合。每个 ECG 数据的长度选择为 20 秒,并对所有 168 = 14 x 12 对数据进行了测试。VF 到 CPR 的比率选择为-20 dB、-15 dB、-10 dB、-5 dB、0 dB、5 dB 和 10 dB。这里-20 dB 对应于 CPR 伪影的最高水平。
对于基于 VF 到 CPR 比率为-20 dB、-15 dB、-10 dB、-5 dB 和 0 dB 的非优化相干线去除,信号到噪声增益(SNR 增益)分别为 9.3 +/- 2.4 dB、9.4 +/- 2.4 dB、9.5 +/- 2.5 dB、9.3 +/- 2.5 dB 和 8.0 +/- 2.7(平均值 +/- 标准差,n = 168)。特征性地,原始 VF 到 CPR 的比率为-10 dB,对应于方差比 var(VF):var(CPR) = 1:10。9.5 dB 的改进导致恢复的 VF 到 CPR 的比率为-0.5 dB,对应于 var(VF):var(CPR) = 1:1.1,信号中 CPR 的方差降低了 8.9 倍。
局部相干线去除算法使用单个 ECG 通道的信息。与多通道算法不同,不需要诸如胸阻抗、血压或 CPR 期间施加在胸骨上的压力等附加信息。包含 CPR 伪影的 VF-ECG 的成功除颤预测因子,例如均值和中位数频率,容易受到伪影谐波的影响。因此,降低 CPR 伪影对于确定成功除颤的估计值的可靠值是必要的。
局部相干线去除算法可减少 VF-ECG 中的 CPR 伪影,但不能完全消除。我们的 SNR 改进与 Rheinberger 等人、Husoy 等人和 Aase 等人的多通道方法提供的改进相当。后两位作者处理的是不同的心室节律(VF 和 VT),而在这里我们只处理 VF。在该算法可以在实际 CPR 情况下进行测试之前,还需要进行进一步的开发。