Department of Radiation Oncology and Molecular Radiation Sciences, Johns Hopkins Hospital, Baltimore, MD, USA.
Ann Surg Oncol. 2010 Apr;17(4):981-90. doi: 10.1245/s10434-009-0743-7. Epub 2010 Jan 20.
Survival for pancreatic ductal adenocarcinoma is low, the role of adjuvant therapy remains controversial, and recent data suggest adjuvant chemoradiation (CRT) may decrease survival compared with surgery alone. Our goal was to examine efficacy of adjuvant CRT in resected pancreatic adenocarcinoma compared with surgery alone.
Patients with pancreatic adenocarcinoma at Johns Hopkins Hospital (n = 794, 1993-2005) and Mayo Clinic (n = 478, 1985-2005) following resection who were observed (n = 509) or received adjuvant 5-FU based CRT (median dose 50.4 Gy; n = 583) were included. Cox survival and propensity score analyses assessed associations with overall survival. Matched-pair analysis by treatment group (1:1) based on institution, age, sex, tumor size/stage, differentiation, margin, and node positivity with N = 496 (n = 248 per treatment arm) was performed.
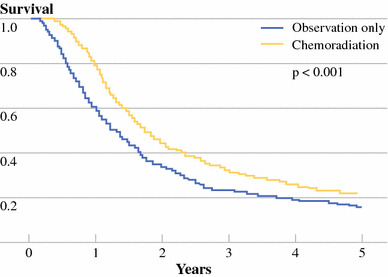
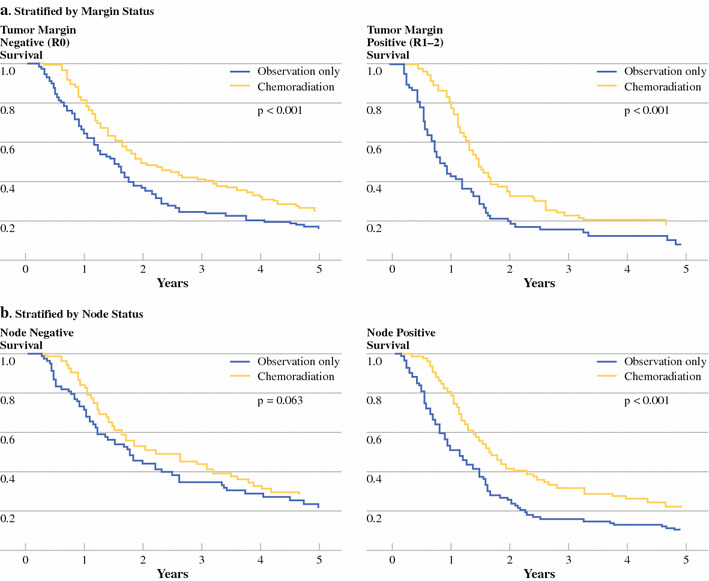
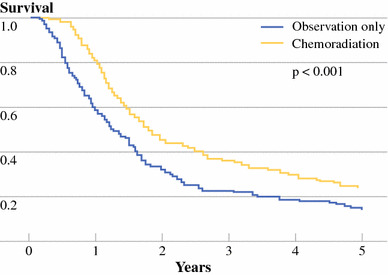
Median survival was 18.8 months. Overall survival (OS) was longer among recipients of CRT versus surgery alone (median survival 21.1 vs. 15.5 months, P < .001; 2- and 5-year OS 44.7 vs. 34.6%; 22.3 vs. 16.1%, P < .001). Compared with surgery alone, adjuvant CRT improved survival in propensity score analysis for all patients by 33% (P < .001), with improved survival when stratified by age, margin, node, and T-stage (RR = 0.57-0.75, P < .05). Matched-pair analysis demonstrated OS was longer with CRT (21.9 vs. 14.3 months median survival; 2- and 5-year OS 45.5 vs. 31.4%; 25.4 vs. 12.2%, P < .001).
Adjuvant CRT is associated with improved survival after pancreaticoduodenectomy. Adjuvant CRT was not associated with decreased survival in any risk group, even in propensity score and matched-pair analyses. Further studies evaluating adjuvant chemotherapy compared with adjuvant chemoradiation are needed to determine the most effective combination of systemic and local-regional therapy to achieve optimal survival results.
胰腺导管腺癌的生存率较低,辅助治疗的作用仍存在争议,最近的数据表明辅助放化疗(CRT)可能会降低与单纯手术相比的生存率。我们的目标是研究与单纯手术相比,辅助 CRT 在切除的胰腺腺癌中的疗效。
在约翰霍普金斯医院(1993-2005 年,n=794)和梅奥诊所(1985-2005 年,n=478)接受切除术的胰腺腺癌患者中,观察(n=509)或接受辅助 5-FU 为基础的 CRT(中位剂量 50.4Gy;n=583)。Cox 生存和倾向评分分析评估了与总生存率的关联。根据机构、年龄、性别、肿瘤大小/分期、分化、切缘和淋巴结阳性情况,采用治疗组(1:1)进行匹配对分析(n=496,每组 248 例)。
中位生存期为 18.8 个月。与单纯手术相比,接受 CRT 治疗的患者总生存率(OS)更长(中位生存期 21.1 个月比 15.5 个月,P<.001;2 年和 5 年 OS 分别为 44.7%比 34.6%;22.3%比 16.1%,P<.001)。与单纯手术相比,辅助 CRT 在所有患者的倾向评分分析中使生存率提高了 33%(P<.001),且在按年龄、切缘、淋巴结和 T 分期分层时,生存率也得到了改善(RR=0.57-0.75,P<.05)。配对分析显示 CRT 组的 OS 更长(中位生存期 21.9 个月比 14.3 个月;2 年和 5 年 OS 分别为 45.5%比 31.4%;25.4%比 12.2%,P<.001)。
辅助 CRT 与胰十二指肠切除术后的生存改善相关。辅助 CRT 并未降低任何风险组的生存率,甚至在倾向评分和配对分析中也是如此。需要进一步研究评估辅助化疗与辅助放化疗的效果,以确定全身治疗与局部区域治疗的最佳联合方案,从而实现最佳的生存结果。