Division of Microbiology and Infectious Diseases, PathWest Laboratory Medicine WA, Queen Elizabeth II Medical Centre, Perth, Western Australia, Australia.
PLoS One. 2010 Jan 14;5(1):e8705. doi: 10.1371/journal.pone.0008705.
Bacterial pneumonia is a well described complication of influenza. In recent years, community-onset methicillin-resistant Staphylococcus aureus (cMRSA) infection has emerged as a contributor to morbidity and mortality in patients with influenza. Since the emergence and rapid dissemination of pandemic A(H1N1)2009 influenzavirus in April 2009, initial descriptions of the clinical features of patients hospitalized with pneumonia have contained few details of patients with bacterial co-infection.
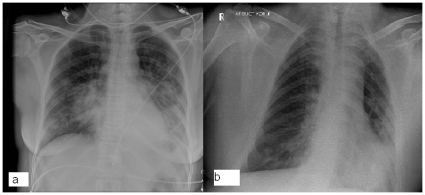
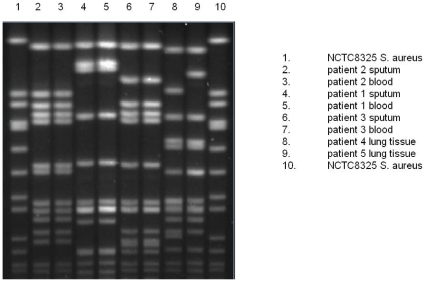
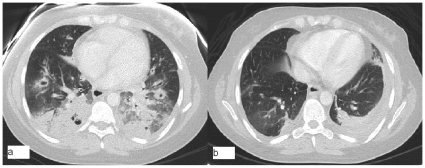
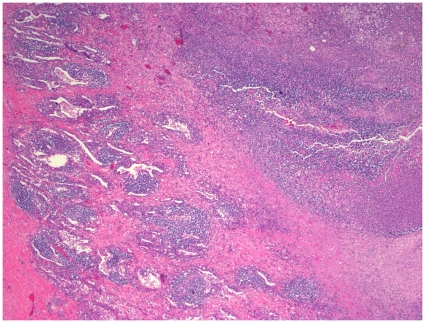
METHODOLOGY/PRINCIPAL FINDINGS: Patients with community-acquired pneumonia (CAP) caused by co-infection with pandemic A(H1N1)2009 influenzavirus and cMRSA were prospectively identified at two tertiary hospitals in one Australian city during July to September 2009, the period of intense influenza activity in our region. Detailed characterization of the cMRSA isolates was performed. 252 patients with pandemic A(H1N1)2009 influenzavirus infection were admitted at the two sites during the period of study. Three cases of CAP due to pandemic A(H1N1)2009/cMRSA co-infection were identified. The clinical features of these patients were typical of those with S. aureus co-infection or sequential infection following influenza. The 3 patients received appropriate empiric therapy for influenza, but inappropriate empiric therapy for cMRSA infection; all 3 survived. In addition, 2 fatal cases of CAP caused by pandemic A(H1N1)2009/cMRSA co-infection were identified on post-mortem examination. The cMRSA infections were caused by three different cMRSA clones, only one of which contained genes for Panton-Valentine Leukocidin (PVL).
CONCLUSIONS/SIGNIFICANCE: Clinicians managing patients with pandemic A(H1N1)2009 influenzavirus infection should be alert to the possibility of co-infection or sequential infection with virulent, antimicrobial-resistant bacterial pathogens such as cMRSA. PVL toxin is not necessary for the development of cMRSA pneumonia in the setting of pandemic A( H1N1) 2009 influenzavirus co-infection.
细菌性肺炎是流感的一种常见并发症。近年来,社区获得性耐甲氧西林金黄色葡萄球菌(cMRSA)感染已成为流感患者发病率和死亡率的一个重要因素。自 2009 年 4 月甲型 H1N1 大流行流感病毒出现并迅速传播以来,最初描述的住院肺炎患者的临床特征很少包含细菌合并感染患者的详细信息。
方法/主要发现:2009 年 7 月至 9 月,在澳大利亚一个城市的两家三级医院,对由大流行甲型 H1N1 2009 流感病毒和 cMRSA 合并感染引起的社区获得性肺炎(CAP)患者进行了前瞻性识别,这是我们地区流感活动剧烈的时期。对 cMRSA 分离株进行了详细的特征描述。在研究期间,这两个地点共收治了 252 例大流行甲型 H1N1 2009 流感病毒感染患者。确定了 3 例由大流行甲型 H1N1 2009/cMRSA 合并感染引起的 CAP 病例。这些患者的临床特征与金黄色葡萄球菌合并感染或流感后继发感染的特征相似。这 3 例患者接受了流感的经验性治疗,但对 cMRSA 感染的经验性治疗不当;所有 3 例患者均存活。此外,在尸检中还发现了 2 例由大流行甲型 H1N1 2009/cMRSA 合并感染引起的致命性 CAP 病例。cMRSA 感染由 3 种不同的 cMRSA 克隆引起,其中只有 1 种含有 Panton-Valentine Leukocidin(PVL)基因。
结论/意义:治疗大流行甲型 H1N1 2009 流感病毒感染患者的临床医生应警惕合并感染或继发感染毒力强、对抗菌药物耐药的细菌病原体(如 cMRSA)的可能性。PVL 毒素不是大流行甲型 H1N1 2009 流感病毒合并感染时 cMRSA 肺炎发生的必要条件。