Cook Joseph, Sur Dipika, Clemens John, Whittington Dale
Evans School of Public Affairs, University of Washington, Seattle, 98195-3055, USA.
J Health Popul Nutr. 2009 Dec;27(6):711-24. doi: 10.3329/jhpn.v27i6.4319.
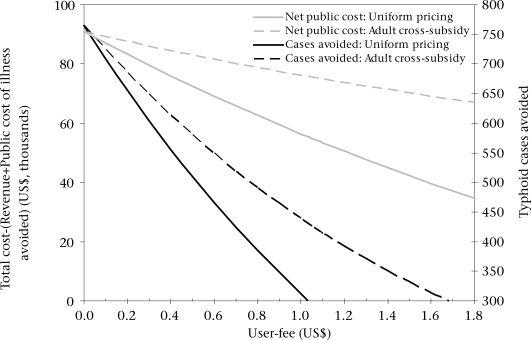
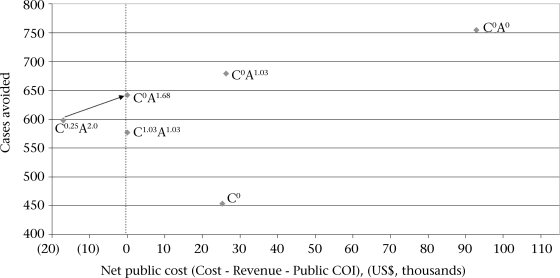
New-generation vaccines against typhoid fever have the potential to reduce the burden of disease in areas where the disease is endemic. The case for public expenditure on typhoid Vi polysaccharide vaccines for two low-income, high-incidence slums (Narkeldanga and Tiljala) in Kolkata, India, was examined. Three measures of the economic benefits of the vaccines were used: private and public cost-of-illness (COI) avoided; avoided COI plus mortality risk-reduction benefits; and willingness-to-pay (WTP) derived from stated preference (contingent valuation) studies conducted in Tiljala in 2004. Benefits and costs were examined from a social perspective. The study represents a unique opportunity to evaluate typhoid-vaccine programmes using a wealth of new site-specific epidemiological and economic data. Three typhoid-vaccination strategies (targeting only enrolled school children, targeting all children, and targeting adults and children) would most likely pass a social cost-benefit test, unless benefits are restricted to include only avoided COI. All three strategies would be considered 'very cost-effective' using the standard comparisons of cost per disability-adjusted life-year avoided with per-capita gross domestic product. However, at an average total cost per immunized person of approximately US$ 1.1, a typhoid-vaccination programme would absorb a sixth of existing public-sector spending on health (on a per-capita basis) in India. Because there appears to be significant private economic demand for typhoid vaccines, the Government could design a financially-sustainable programme with user-fees. The results show that a programme where adults pay a higher fee to subsidize vaccines for children (who have higher incidence) would avoid more cases than a uniform user-fee and still achieve revenue-neutrality.
新一代伤寒疫苗有潜力减轻疾病流行地区的疾病负担。本文考察了在印度加尔各答两个低收入、高发病率贫民窟(纳克尔丹加和蒂尔贾拉)为伤寒Vi多糖疫苗提供公共支出的理由。使用了三种衡量疫苗经济效益的方法:避免的私人和公共疾病成本(COI);避免的COI加上降低死亡风险的益处;以及从2004年在蒂尔贾拉进行的陈述偏好(条件估值)研究得出的支付意愿(WTP)。从社会角度审视了收益和成本。这项研究提供了一个独特的机会,可利用大量新的特定地点流行病学和经济数据来评估伤寒疫苗计划。三种伤寒疫苗接种策略(仅针对入学儿童、针对所有儿童以及针对成人和儿童)很可能通过社会成本效益测试,除非收益仅限于避免的COI。使用避免的每伤残调整生命年成本与人均国内生产总值的标准比较,所有这三种策略都将被视为“非常具有成本效益”。然而,伤寒疫苗接种计划每位接种者的平均总成本约为1.1美元,这将占印度现有公共部门人均卫生支出的六分之一。由于对伤寒疫苗似乎存在巨大的私人经济需求,政府可以设计一项收取用户费用且财务上可持续的计划。结果表明,与统一收取用户费用相比,一项让成年人支付更高费用以补贴儿童(发病率更高)疫苗的计划能够避免更多病例,并且仍能实现收支平衡。