Department of Surgery, The Ohio State University, Columbus, OH, USA.
Ann Surg Oncol. 2010 Apr;17(4):991-7. doi: 10.1245/s10434-009-0883-9. Epub 2010 Jan 28.
Cancers of the ampulla of Vater, distal common bile duct, and pancreas are known to have dismal prognosis. It is often reported that ampullary cancers are less aggressive relative to the other periampullary carcinomas. We sought to evaluate predictors of survival for periampullary cancers following pancreaticoduodenectomy to identify biologic behavior.
We reviewed the records of all patients who underwent pancreaticoduodenectomy for periampullary carcinoma between 1992 and 2007 at the Ohio State University Medical Center. Demographics, treatment, and outcome/survival data were analyzed. Kaplan-Meier survival curves were created and compared by log-rank analysis. Multivariate analysis was undertaken using Cox proportional-hazards method.
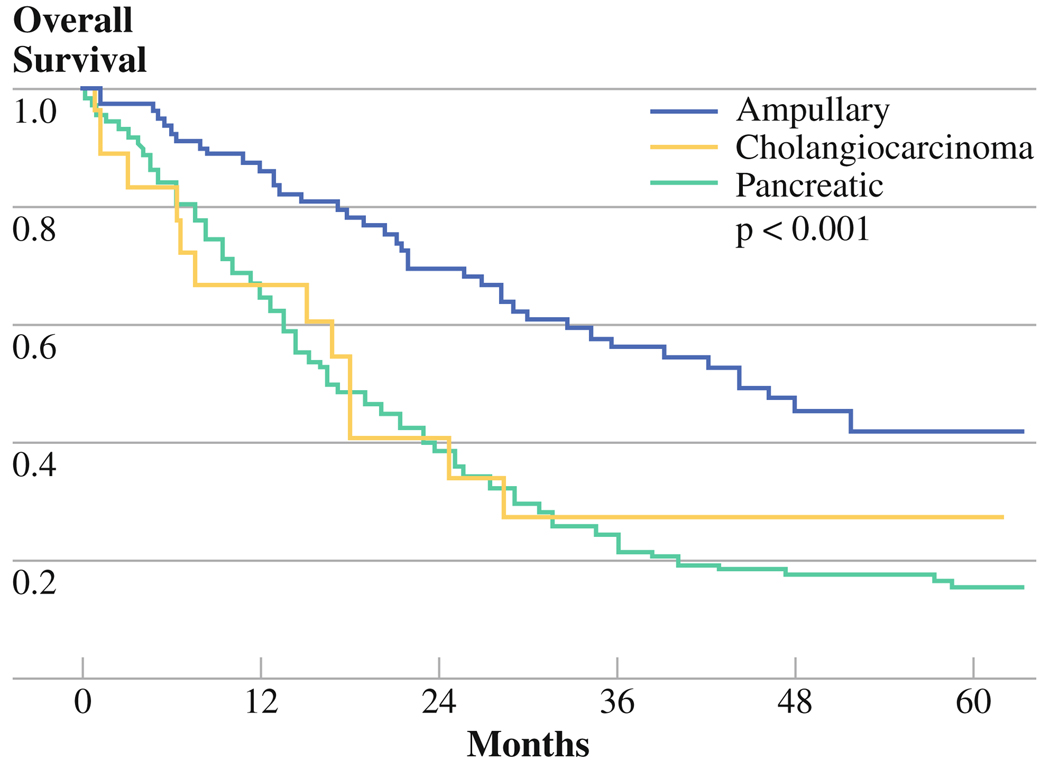
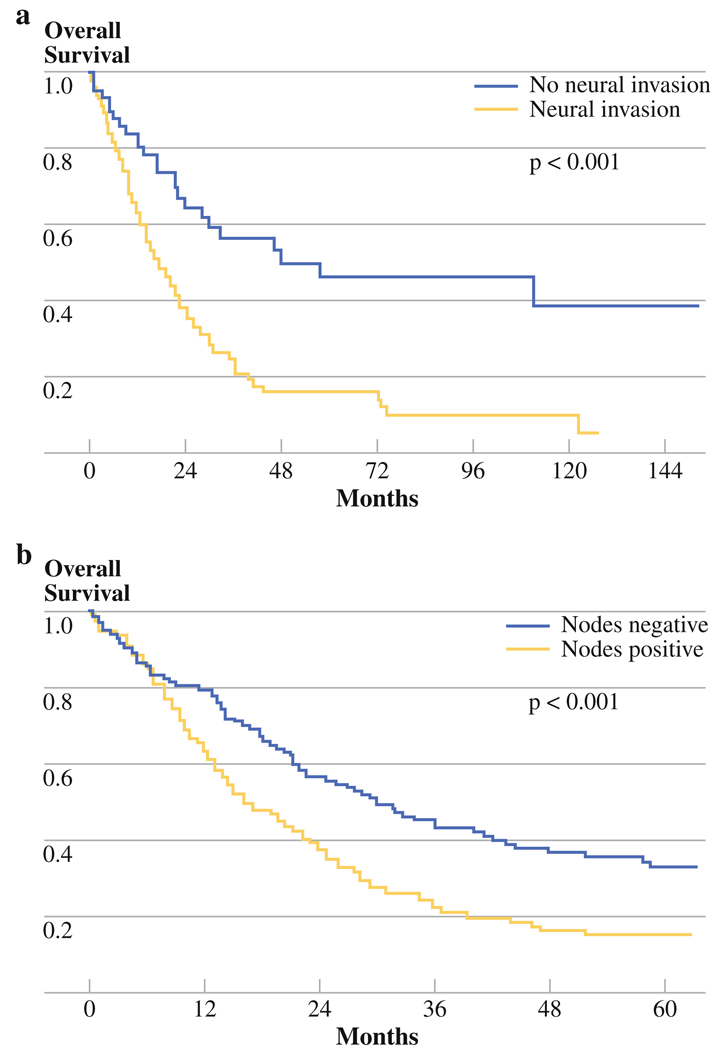
346 consecutive periampullary malignancies (249 pancreatic cancers, 79 ampullary carcinomas, 18 extrahepatic cholangiocarcinomas) treated by pancreaticoduodenectomy were identified. Pancreatic cancer histology correlated with the shortest median survival (17.1 months), followed by cholangiocarcinoma (17.9 months) and ampullary carcinoma (44.3 months) (P < 0.001). Potential predictors of decreased survival on univariate analysis included site of origin, preoperative jaundice, microscopic positive margin, nodal metastasis, lymphovascular invasion, neural invasion, and poor differentiation. Only nodal metastasis (median 16.2 versus 29.9 months, P < 0.001) and neural invasion (median 17.7 versus 47.9 months, P < 0.00001) significantly predicted outcome on multivariate analysis.
Although ampullary cancers have the best prognosis overall, when controlled for tumor stage, only presence of neural invasion and nodal metastasis predict poor survival following pancreaticoduodenectomy. Biological behavior remains the most important prognostic indicator in periampullary cancers amenable to resection, regardless of site of origin.
Vater 壶腹、远端胆总管和胰腺的癌症预后通常较差。据报道,相对于其他壶腹周围癌,壶腹癌的侵袭性较小。我们试图评估胰十二指肠切除术后壶腹周围癌的生存预测因素,以确定其生物学行为。
我们回顾了 1992 年至 2007 年间在俄亥俄州立大学医疗中心接受胰十二指肠切除术治疗的所有壶腹周围癌患者的记录。分析了人口统计学、治疗和结果/生存数据。通过对数秩分析创建和比较 Kaplan-Meier 生存曲线。使用 Cox 比例风险方法进行多变量分析。
确定了 346 例连续的壶腹周围恶性肿瘤(249 例胰腺癌、79 例壶腹癌、18 例肝外胆管癌),通过胰十二指肠切除术治疗。胰腺癌组织学与最短的中位生存期相关(17.1 个月),其次是胆管癌(17.9 个月)和壶腹癌(44.3 个月)(P < 0.001)。单因素分析中潜在的生存预测因素包括起源部位、术前黄疸、显微镜下阳性切缘、淋巴结转移、淋巴血管侵犯、神经侵犯和低分化。只有淋巴结转移(中位 16.2 个月与 29.9 个月,P < 0.001)和神经侵犯(中位 17.7 个月与 47.9 个月,P < 0.00001)在多因素分析中显著预测了结果。
尽管壶腹癌总体预后最好,但在控制肿瘤分期后,只有神经侵犯和淋巴结转移预测胰十二指肠切除术后生存不良。生物学行为仍然是可切除的壶腹周围癌最重要的预后指标,与起源部位无关。