Department of Cardiology, Copenhagen University Hospital Gentofte, Niels Andersens Vej 65, 2900 Hellerup, Denmark.
BMC Cardiovasc Disord. 2010 Jan 29;10:6. doi: 10.1186/1471-2261-10-6.
The optimal duration of clopidogrel treatment after percutaneous coronary intervention (PCI) is unclear. We studied the risk of death or recurrent myocardial infarction (MI) in relation to 6- and 12-months clopidogrel treatment among MI patients treated with PCI.
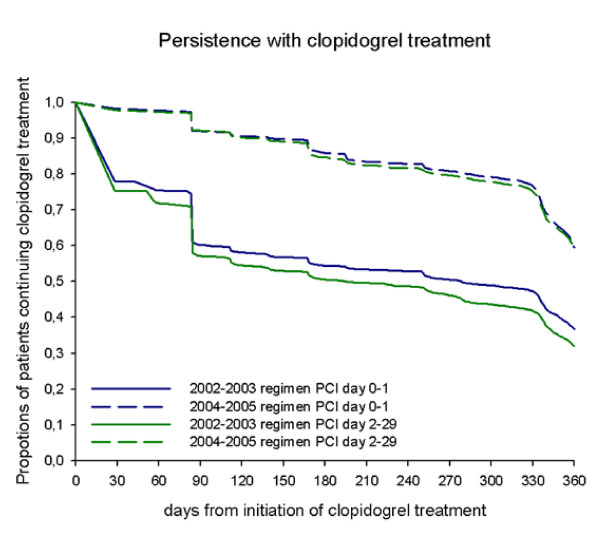
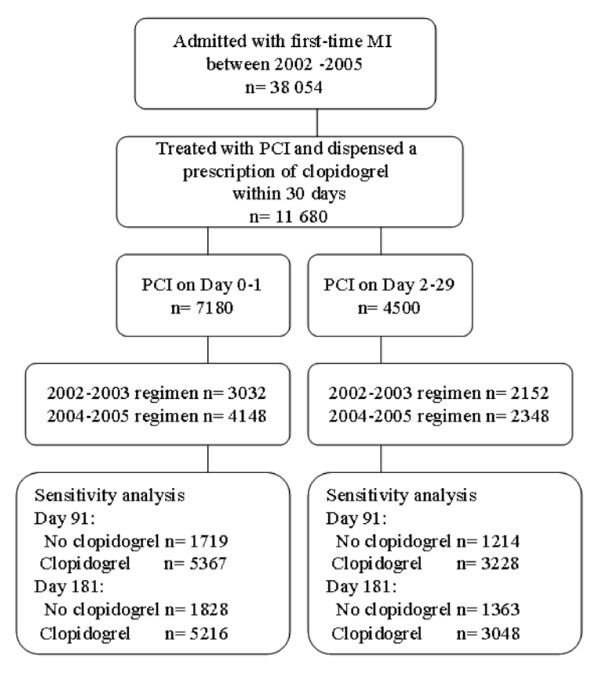
Using nationwide registers of hospitalizations and drug dispensing from pharmacies we identified 11 680 patients admitted with MI, treated with PCI and clopidogrel. Clopidogrel treatment was categorized in a 6-months and a 12-months regimen. Rates of death, recurrent MI or a combination of both were analyzed by the Kaplan Meier method and Cox proportional hazards models. Bleedings were compared between treatment regimens.
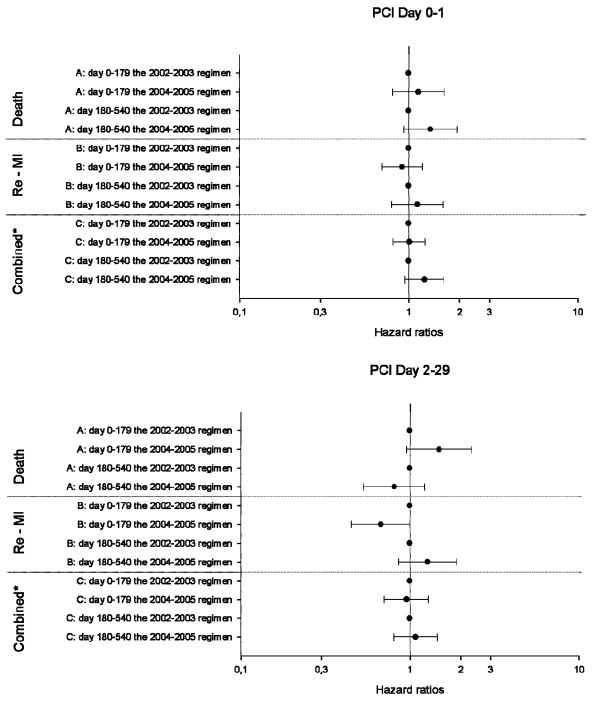
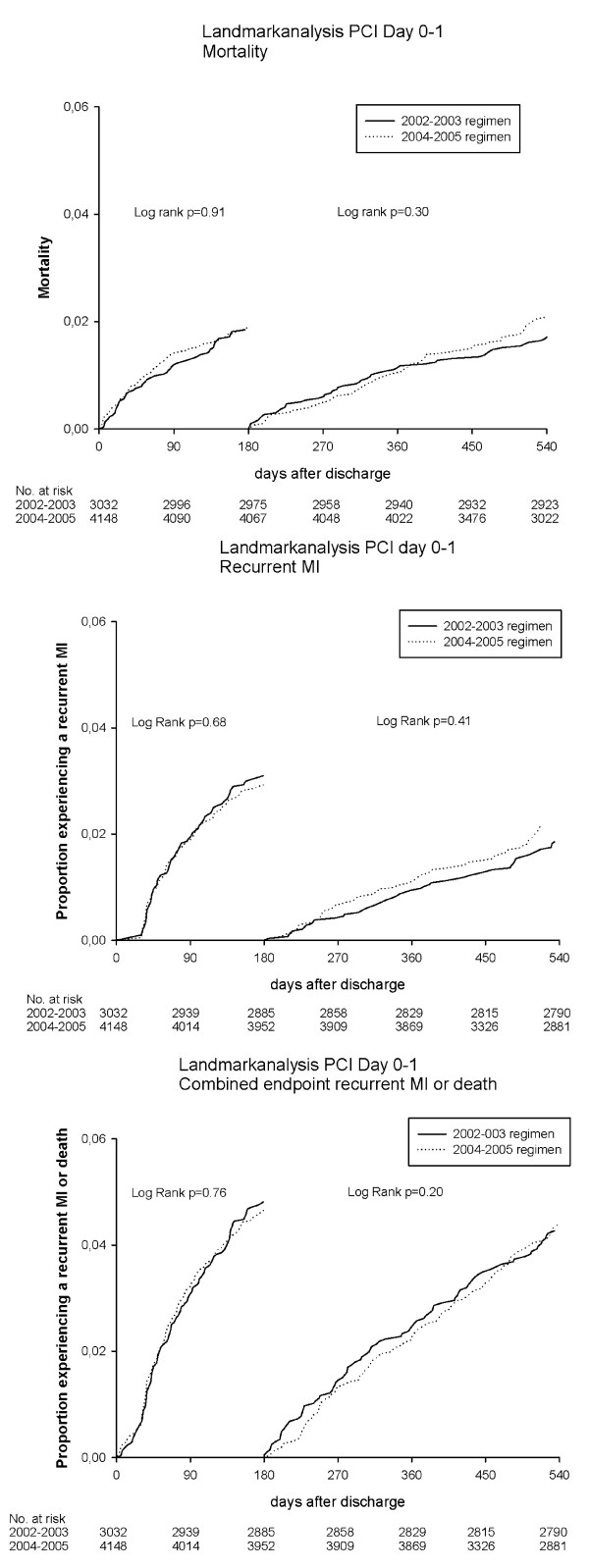
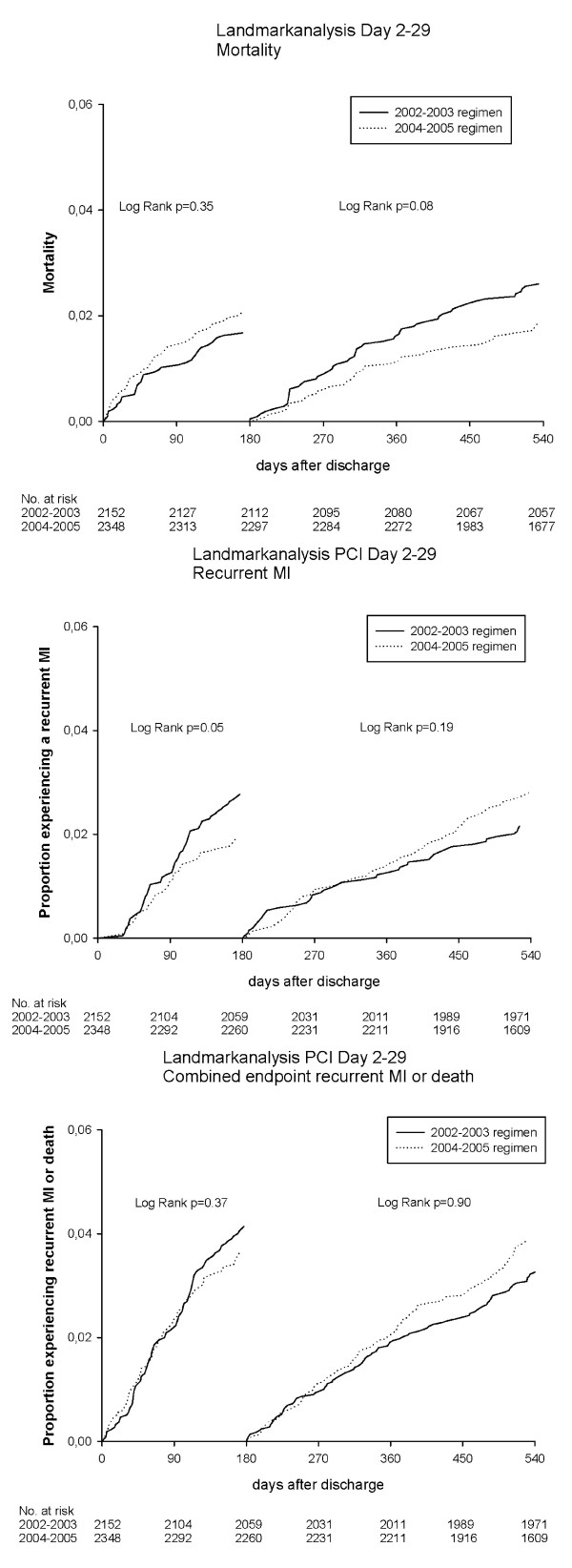
The Kaplan Meier analysis indicated no benefit of the 12-months regimen compared with the 6-months in all endpoints. The Cox proportional hazards analysis confirmed these findings with hazard ratios for the 12-months regimen (the 6-months regimen used as reference) for the composite endpoint of 1.01 (confidence intervals 0.81-1.26) and 1.24 (confidence intervals 0.95-1.62) for Day 0-179 and Day 180-540 after discharge. Bleedings occurred in 3.5% and 4.1% of the patients in the 6-months and 12-months regimen (p = 0.06).
We found comparable rates of death and recurrent MI in patients treated with 6- and 12-months' clopidogrel. The potential benefit of prolonged clopidogrel treatment in a real-life setting remains uncertain.
经皮冠状动脉介入治疗(PCI)后氯吡格雷治疗的最佳持续时间尚不清楚。我们研究了 PCI 治疗的 MI 患者中,6 个月和 12 个月氯吡格雷治疗与死亡或再发心肌梗死(MI)风险的关系。
我们使用全国住院和药房药物配给登记处,确定了 11680 例 MI 患者,这些患者接受了 PCI 和氯吡格雷治疗。氯吡格雷治疗分为 6 个月和 12 个月疗程。通过 Kaplan-Meier 法和 Cox 比例风险模型分析死亡率、再发 MI 或两者兼有的发生率。比较了两种治疗方案的出血情况。
Kaplan-Meier 分析表明,在所有终点中,与 6 个月相比,12 个月方案没有获益。Cox 比例风险分析证实了这一发现,对于复合终点,12 个月方案的危险比(6 个月方案作为参考)为 1.01(置信区间 0.81-1.26)和 1.24(置信区间 0.95-1.62),分别为出院后第 0-179 天和第 180-540 天。6 个月和 12 个月方案的患者出血发生率分别为 3.5%和 4.1%(p=0.06)。
我们发现,6 个月和 12 个月氯吡格雷治疗的患者死亡率和再发 MI 发生率相当。在真实环境中,延长氯吡格雷治疗的潜在获益仍不确定。