Department of Public Health, Erasmus Medical Center, PO Box 2040, 3000 CA Rotterdam, the Netherlands.
J Natl Cancer Inst. 2010 Mar 3;102(5):352-5. doi: 10.1093/jnci/djp533. Epub 2010 Feb 8.
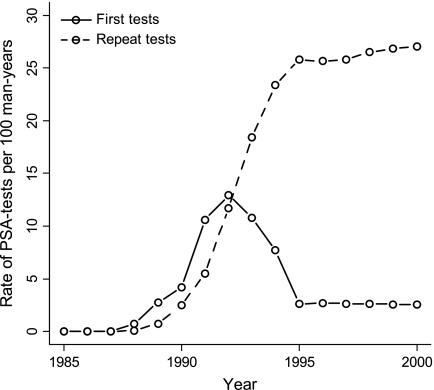
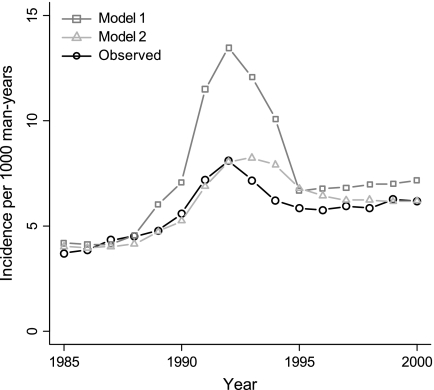
Dissemination of prostate-specific antigen (PSA) testing in the United States coincided with an increasing incidence of prostate cancer, a shift to earlier stage disease at diagnosis, and decreasing prostate cancer mortality. We compared PSA screening performance with respect to prostate cancer detection in the US population vs in the Rotterdam section of the European Randomized Study of Screening for Prostate Cancer (ERSPC-Rotterdam). We developed a simulation model for prostate cancer and PSA screening for ERSPC-Rotterdam. This model was then adapted to the US population by replacing demography parameters with US-specific ones and the screening protocol with the frequency of PSA tests in the US population. We assumed that the natural progression of prostate cancer and the sensitivity of a PSA test followed by a biopsy were the same in the United States as in ERSPC-Rotterdam. The predicted prostate cancer incidence peak in the United States was then substantially higher than the observed prostate cancer incidence peak (13.3 vs 8.1 cases per 1000 man-years). However, the actual observed incidence was reproduced by assuming a substantially lower PSA test sensitivity in the United States than in ERSPC-Rotterdam. For example, for nonpalpable local- or regional-stage cancers (ie, stage T1M0), the estimates of PSA test sensitivity were 0.26 in the United States vs 0.94 in ERSPC-Rotterdam. We conclude that the efficacy of PSA screening in detecting prostate cancer was lower in the United States than in ERSPC-Rotterdam.
在美国,前列腺特异性抗原(PSA)检测的传播与前列腺癌发病率的增加、诊断时疾病向早期阶段的转移以及前列腺癌死亡率的降低同时发生。我们比较了 PSA 筛查在检测美国人群和欧洲前列腺癌筛查随机研究(ERSPC-Rotterdam)的 Rotterdam 部分的前列腺癌方面的表现。我们为 ERSPC-Rotterdam 开发了一种前列腺癌和 PSA 筛查的模拟模型。然后,通过用美国特有的人口统计学参数替换人口统计学参数,并将筛查方案替换为美国人群中的 PSA 检测频率,使该模型适应美国人群。我们假设前列腺癌的自然进展和随后进行活检的 PSA 检测的敏感性在美国与 ERSPC-Rotterdam 相同。然后,美国预测的前列腺癌发病率高峰远高于实际观察到的前列腺癌发病率高峰(美国为每 1000 人年 13.3 例,而 ERSPC-Rotterdam 为 8.1 例)。然而,通过假设美国的 PSA 检测敏感性明显低于 ERSPC-Rotterdam,实际观察到的发病率得到了重现。例如,对于不可触及的局部或区域阶段癌症(即 T1M0 期),PSA 检测敏感性的估计值在美国为 0.26,而在 ERSPC-Rotterdam 为 0.94。我们的结论是,PSA 筛查在检测前列腺癌方面的效果在美国低于 ERSPC-Rotterdam。