Department of Radiation Oncology, The University of Oklahoma Health Sciences Center, Oklahoma City, OK 73104, USA.
J Appl Clin Med Phys. 2010 Jan 29;11(1):3133. doi: 10.1120/jacmp.v11i1.3133.
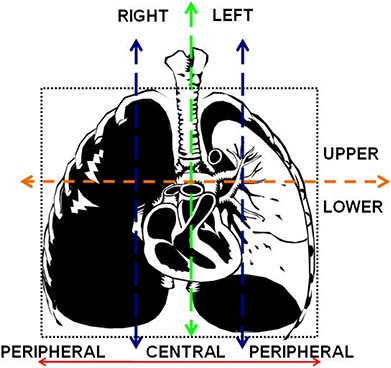
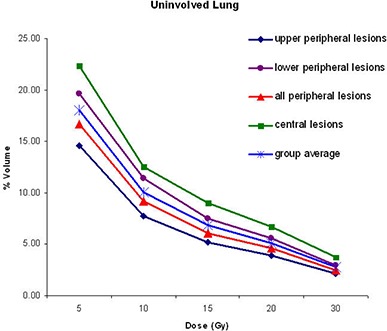
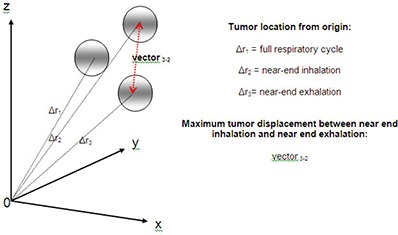
The purpose of this study was to assess the impact of respiratory gating on tumor and normal tissue dosimetry in patients treated with SBRT for early stage non-small cell lung cancer (NSCLC). Twenty patients with stage I NSCLC were studied. Treatment planning was performed using four-dimensional computed tomography (4D CT) with free breathing (Plan I), near-end inhalation (Plan II), and near-end exhalation (Plan III). The prescription dose was 60 Gy in three fractions. The tumor displacement was most pronounced for lower peripheral lesions (average 7.0 mm, range 4.1-14.3 mm) when compared to upper peripheral (average 2.4mm, range 1.0-5.1 mm) or central lesions (average 2.9 mm, range 1.0-4.1 mm). In this study, the pencil beam convolution (PBC) algorithm with modified Batho power law for tissue heterogeneity was used for dose calculation. There were no significant differences in tumor and normal tissue dosimetry among the three gated plans. Tumor location however, significantly influenced tumor doses because of the necessity of respecting normal tissue constraints of centrally located structures. For plans I, II and III, average doses to central lesions were lower as compared with peripheral lesions by 4.88 Gy, 8.24 Gy and 6.93 Gy for minimum PTV and 0.98, 1.65 and 0.87 Gy for mean PTV dose, respectively. As a result, the mean single fraction equivalent dose (SFED) values were also lower for central compared to peripheral lesions. In addition, central lesions resulted in higher mean doses for lung, esophagus, and ipsilateral bronchus by 1.24, 1.93 and 7.75 Gy, respectively. These results indicate that the tumor location is the most important determinant of dosimetric optimization of SBRT plans. Respiratory gating proved unhelpful in the planning of these patients with severe COPD.
本研究旨在评估在接受早期非小细胞肺癌(NSCLC)立体定向体部放疗(SBRT)的患者中,呼吸门控对肿瘤和正常组织剂量学的影响。研究了 20 例 I 期 NSCLC 患者。使用自由呼吸(Plan I)、近吸气末(Plan II)和近呼气末(Plan III)的四维 CT(4D CT)进行治疗计划。处方剂量为 60Gy,分 3 次。与上外周(平均 2.4mm,范围 1.0-5.1mm)或中央病变(平均 2.9mm,范围 1.0-4.1mm)相比,下外周病变的肿瘤位移最为明显(平均 7.0mm,范围 4.1-14.3mm)。在这项研究中,使用了带有组织不均匀性修正 Batho 幂律的笔束卷积(PBC)算法进行剂量计算。在三个门控计划中,肿瘤和正常组织的剂量学没有显著差异。然而,由于需要尊重中央结构的正常组织限制,肿瘤位置显著影响肿瘤剂量。对于计划 I、II 和 III,中央病变的平均剂量分别比外周病变低 4.88Gy、8.24Gy 和 6.93Gy,对于最小 PTV;0.98Gy、1.65Gy 和 0.87Gy,对于平均 PTV 剂量。因此,中央病变的平均单次分割等效剂量(SFED)值也比外周病变低。此外,中央病变使肺、食管和同侧支气管的平均剂量分别增加 1.24Gy、1.93Gy 和 7.75Gy。这些结果表明,肿瘤位置是 SBRT 计划剂量优化的最重要决定因素。呼吸门控在这些严重 COPD 患者的计划中没有帮助。