Barber John Ck, Bunyan Dave, Curtis Merryl, Robinson Denise, Morlot Susanne, Dermitzel Anette, Liehr Thomas, Alves Claudia, Trindade Joana, Paramos Ana I, Cooper Clare, Ocraft Kevin, Taylor Emma-Jane, Maloney Viv K
Wessex Regional Genetics Laboratory, Salisbury NHS Foundation Trust, Salisbury, SP2 8BJ, UK.
Mol Cytogenet. 2010 Feb 18;3:3. doi: 10.1186/1755-8166-3-3.
The 8p23.1 duplication syndrome and copy number variation of the 8p23.1 defensin gene cluster are cytogenetically indistinguishable but distinct at the molecular level. To our knowledge, the 8p23.1 duplication syndrome has been described at prenatal diagnosis only once and we report our experience with four further apparent duplications ascertained at prenatal diagnosis.
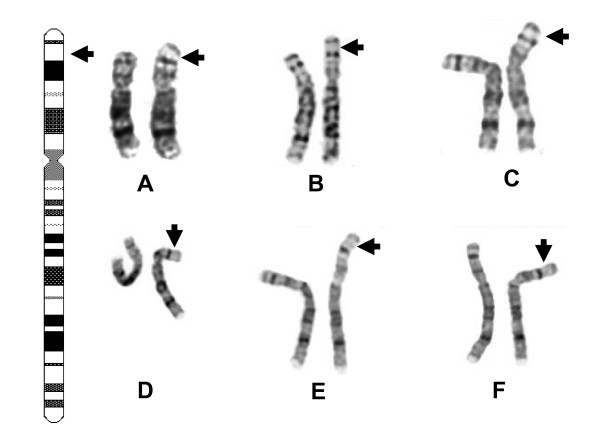
Additional material at band 8p23.1 was detected using conventional G-banded cytogenetics in each case. Multiplex Ligation-dependent Probe Amplification (MLPA) or Fluorescence In Situ Hybridisation (FISH) were used depending on whether only DNA (Cases 1 and 4) or cytogenetic preparations (Cases 2 and 3) were available from the laboratory of origin. The extent of the duplication in Case 1 was retrospectively determined using array Comparative Genomic Hybridisation (array CGH).
Three cases of 8p23.1 duplication syndrome were found (Cases 1 to 3). Two were de novo and continued to term and the third, a paternally transmitted duplication, was terminated because of a previous child with psychomotor delay and 8p23.1 duplication syndrome. Case 1 was ascertained with a hypoplastic left heart but the ventricular septal and interventricular defects, in Cases 2 and 3 respectively, were found after ascertainment for advanced maternal age. By contrast, case 4 was a maternally transmitted copy number variation of the defensin cluster with normal outcome.
Our data underline the need to differentiate 8p23.1 duplications from copy number variation of the defensin cluster using FISH, MLPA or array CGH. Cardiac defects were ascertained by ultrasound in only one of the three duplication 8p23.1 pregnancies but were visible in two of the three at 21 to 22 weeks gestation. Our results provide further evidence that both deletion and duplication of the GATA4 transcription factor can give rise to a variety of conotruncal heart defects with variable penetrance and expressivity.
8p23.1重复综合征与8p23.1防御素基因簇的拷贝数变异在细胞遗传学上难以区分,但在分子水平上有所不同。据我们所知,8p23.1重复综合征仅在产前诊断时有过一次报道,我们报告另外4例在产前诊断时确定的明显重复病例的经验。
在每个病例中使用传统的G显带细胞遗传学检测8p23.1带的额外物质。根据原始实验室是否仅有DNA(病例1和4)或细胞遗传学标本(病例2和3),分别使用多重连接依赖探针扩增(MLPA)或荧光原位杂交(FISH)。病例1中重复的范围通过阵列比较基因组杂交(阵列CGH)进行回顾性确定。
发现3例8p23.1重复综合征(病例1至3)。2例为新发,继续妊娠至足月,第3例为父系遗传的重复,因前一个孩子有精神运动发育迟缓及8p23.1重复综合征而终止妊娠。病例1因左心发育不全确诊,而病例2和3分别因高龄产妇确诊,之后发现室间隔和心室间缺损。相比之下,病例4是母系遗传的防御素基因簇拷贝数变异,结局正常。
我们的数据强调需要使用FISH、MLPA或阵列CGH将8p23.1重复与防御素基因簇的拷贝数变异区分开来。在3例8p23.1重复的妊娠中,仅1例通过超声确诊有心脏缺陷,但在妊娠21至22周时,3例中有2例可见心脏缺陷。我们的结果进一步证明,GATA4转录因子的缺失和重复均可导致多种具有不同外显率和表达度的圆锥动脉干心脏缺陷。