Pediatric Immunohaematology and Bone Marrow Transplantation Unit, San Raffaele Scientific Institute, Milan, Italy.
Ital J Pediatr. 2010 Feb 6;36:14. doi: 10.1186/1824-7288-36-14.
Neurotoxicity is a recognized complication of cyclosporine A (CSA) treatment. The incidence of severe CSA-related neurological complications following hematopoietic stem cell transplantation (HSCT) is 4-11%.
We describe 6 cases of CSA related neurotoxicity out of 67 matched related HSCT performed in paediatric Middle East patients affected by haemoglobinopaties (5 beta thalassemia major, 1 sickle cell disease-SCD). Conditioning regimen consisted of iv busulphan, cyclophosphamide and graft-versus-host-disease (GvHD) prophylaxis with CSA, methylprednisolone, methotrexate and ATG.
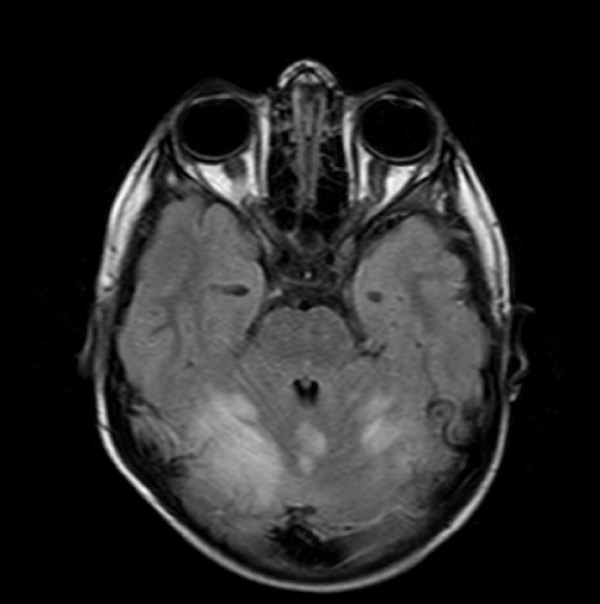
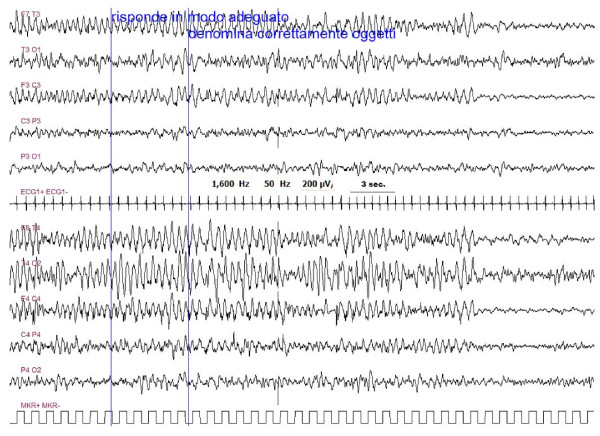
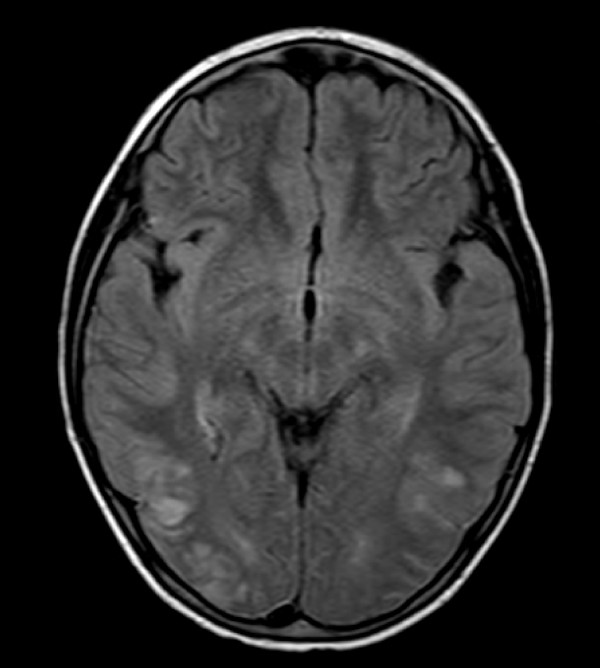
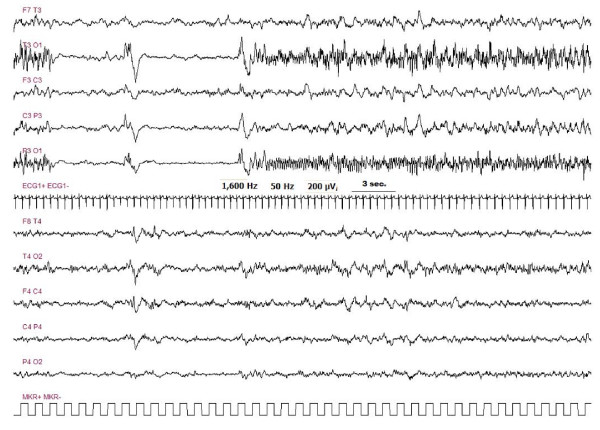
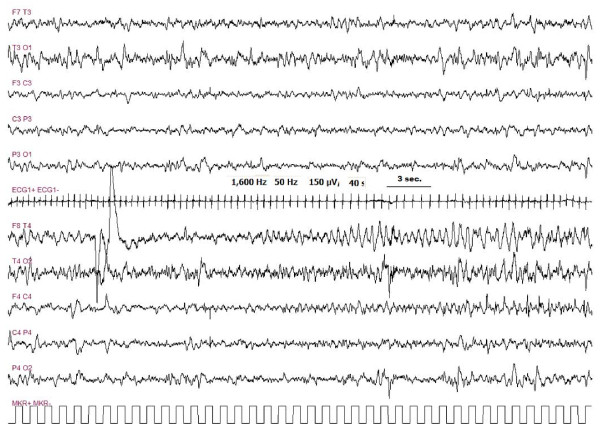
All 6 patients presented prodromes such as arterial hypertension, headache, visual disturbances and vomiting, one to two days before overt CSA neurotoxicity. CSA neurotoxicity consisted of generalized seizures, signs of endocranial hypertension and visual disturbances at a median day of onset of 11 days after HSCT (range +1 to +40). Brain magnetic resonance imaging (MRI) performed in all subjects showed reversible leukoencephalopathy predominantly in the posterior regions of the brain (PRES) in 5/6 patients. EEG performed in 5/6 patients was always abnormal. Neurotoxicity was not explainable by high CSA blood levels, as all patients had CSA in the therapeutic range with a median of 178 ng/ml (range 69-250). CSA was promptly stopped and switched to tacrolimus with disappearance of clinical and radiological findings. All patients are symptoms-free at a median follow up of 882 days (range 60-1065).
Our experience suggests that paediatric patients with haemoglobinopaties have a high incidence of CSA related neurological events with no correlation between serum CSA levels and neurotoxicity. Prognosis is good following CSA removal. Specific prodromes such as arterial hypertension, headache or visual disturbances occurring in the early post-transplant period should be carefully evaluated with electrophysiological and MRI-based imaging in order to intervene promptly and avoid irreversible sequels.
神经毒性是环孢素 A(CSA)治疗的公认并发症。造血干细胞移植(HSCT)后严重 CSA 相关神经并发症的发生率为 4-11%。
我们描述了 6 例 CSA 相关神经毒性病例,这些病例来自中东儿童患者的 HSCT,这些患者患有血红蛋白病(5β地中海贫血,1 例镰状细胞病-SCD)。预处理方案包括静脉注射白消安、环磷酰胺和 CSA、甲基强的松龙、甲氨蝶呤和 ATG 预防移植物抗宿主病(GvHD)。
所有 6 例患者在 CSA 神经毒性明显之前的 1-2 天出现前驱症状,如高血压、头痛、视力障碍和呕吐。CSA 神经毒性表现为全身性癫痫发作、颅内压升高的体征和视觉障碍,发病中位时间为 HSCT 后 11 天(范围+1 至+40)。所有患者的脑磁共振成像(MRI)显示 5/6 例患者主要在后脑区域可逆性白质脑病(PRES)。5/6 例患者的脑电图(EEG)始终异常。CSA 神经毒性不能用高 CSA 血药浓度来解释,因为所有患者的 CSA 均处于治疗范围内,中位数为 178ng/ml(范围 69-250)。CSA 被迅速停用并换用他克莫司,临床和放射学发现消失。所有患者在中位随访 882 天(范围 60-1065)时无任何症状。
我们的经验表明,血红蛋白病患儿 CSA 相关神经事件的发生率较高,血清 CSA 水平与神经毒性无相关性。CSA 去除后预后良好。在移植后早期出现的高血压、头痛或视觉障碍等特定前驱症状应通过电生理和基于 MRI 的影像学进行仔细评估,以便及时干预,避免不可逆的后遗症。