Vretzakis George, Kleitsaki Athina, Stamoulis Konstantinos, Bareka Metaxia, Georgopoulou Stavroula, Karanikolas Menelaos, Giannoukas Athanasios
Cardiac Anesthesia Unit, Department of Anesthesiology, University Hospital of Larissa, Greece.
J Cardiothorac Surg. 2010 Feb 24;5:7. doi: 10.1186/1749-8090-5-7.
Cardiac surgery is a major consumer of blood products, and hemodilution increases transfusion requirements during cardiac surgery under CPB. As intraoperative parenteral fluids contribute to hemodilution, we evaluated the hypothesis that intraoperative fluid restriction reduces packed red-cell (PRC) use, especially in transfusion-prone adults undergoing elective cardiac surgery.
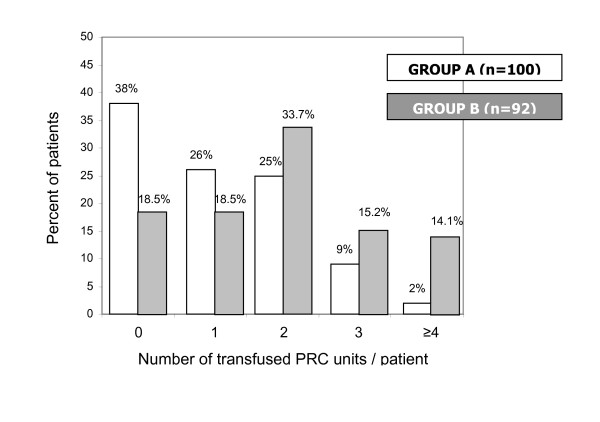
192 patients were randomly assigned to restrictive (group A, 100 pts), or liberal (group B, 92 pts) intraoperative intravenous fluid administration. All operations were conducted by the same team (same surgeon and perfusionist). After anesthesia induction, intravenous fluids were turned off in Group A (fluid restriction) patients, who only received fluids if directed by protocol. In contrast, intravenous fluid administration was unrestricted in group B. Transfusion decisions were made by the attending anesthesiologist, based on identical transfusion guidelines for both groups.
137 of 192 patients received 289 PRC units in total. Age, sex, weight, height, BMI, BSA, LVEF, CPB duration and surgery duration did not differ between groups. Fluid balance was less positive in Group A. Fewer group A patients (62/100) required transfusion compared to group B (75/92, p < 0.04). Group A patients received fewer PRC units (113) compared to group B (176; p < 0.0001). Intraoperatively, the number of transfused units and transfused patients was lower in group A (31 u in 19 pts vs. 111 u in 62 pts; p < 0.001). Transfusions in ICU did not differ significantly between groups. Transfused patients had higher age, lower weight, height, BSA and preoperative hematocrit, but no difference in BMI or discharge hematocrit. Group B (p < 0.005) and female gender (p < 0.001) were associated with higher transfusion probability. Logistic regression identified group and preoperative hematocrit as significant predictors of transfusion.
Our data suggest that fluid restriction reduces intraoperative PRC transfusions without significantly increasing postoperative transfusions in cardiac surgery; this effect is more pronounced in transfusion-prone patients.
NCT00600704, at the United States National Institutes of Health.
心脏手术是血液制品的主要消耗途径,而血液稀释会增加体外循环(CPB)下心脏手术期间的输血需求。由于术中肠外补液会导致血液稀释,我们评估了术中限制补液可减少浓缩红细胞(PRC)使用量的假设,尤其是在接受择期心脏手术且容易输血的成年人中。
192例患者被随机分配至术中静脉补液限制组(A组,100例)或自由补液组(B组,92例)。所有手术均由同一团队(同一位外科医生和灌注师)进行。麻醉诱导后,A组(补液限制组)患者停止静脉补液,仅在方案指示下接受补液。相比之下,B组静脉补液不受限制。输血决策由主治麻醉医生根据两组相同的输血指南做出。
192例患者中的137例共接受了289个PRC单位的输血。两组患者的年龄、性别、体重、身高、BMI、体表面积(BSA)、左心室射血分数(LVEF)、CPB持续时间和手术持续时间无差异。A组的液体平衡阳性程度较低。与B组(75/92)相比,A组需要输血的患者较少(62/1百)(p<0.04)。A组患者接受的PRC单位少于B组(113个 vs. 176个;p<0.0001)。术中,A组的输血量和输血患者数量较低(19例患者输31单位 vs. 62例患者输111单位;p<0.001)。两组在重症监护病房(ICU)的输血量无显著差异。输血患者的年龄较大、体重、身高、BSA和术前血细胞比容较低,但BMI或出院时血细胞比容无差异。B组(p<0.005)和女性(p<0.001)与较高的输血概率相关。逻辑回归分析确定分组和术前血细胞比容是输血的重要预测因素。
我们的数据表明,在心脏手术中,限制补液可减少术中PRC输血,且不会显著增加术后输血;这种效果在容易输血的患者中更为明显。
美国国立卫生研究院,NCT(00600704)。