Hospital Alemão Oswaldo Cruz, Departamento de Medicina Intensiva, São Paulo, SP, Brazil.
Friedrich-Schiller-University, Department of Anaesthesiology and Intensive Care Medicine, Jena, Germany.
Braz J Anesthesiol. 2022 Nov-Dec;72(6):688-694. doi: 10.1016/j.bjane.2022.07.006. Epub 2022 Jul 30.
Recent data suggest the regime of fluid therapy intraoperatively in patients undergoing major surgeries may interfere in patient outcomes. The development of postoperative Acute Kidney Injury (AKI) has been associated with both Restrictive Fluid Balance (RFB) and Liberal Fluid Balance (LFB) during non-cardiac surgery. In patients undergoing cardiac surgery, this influence remains unclear. The study objective was to evaluate the relationship between intraoperative RFB vs. LFB and the incidence of Cardiac-Surgery-Associated AKI (CSA-AKI) and major postoperative outcomes in patients undergoing on-pump Coronary Artery Bypass Grafting (CABG).
This prospective, multicenter, observational cohort study was set at two high-complexity university hospitals in Brazil. Adult patients who required postoperative intensive care after undergoing elective on-pump CABG were allocated to two groups according to their intraoperative fluid strategy (RFB or LFB) with no intervention.
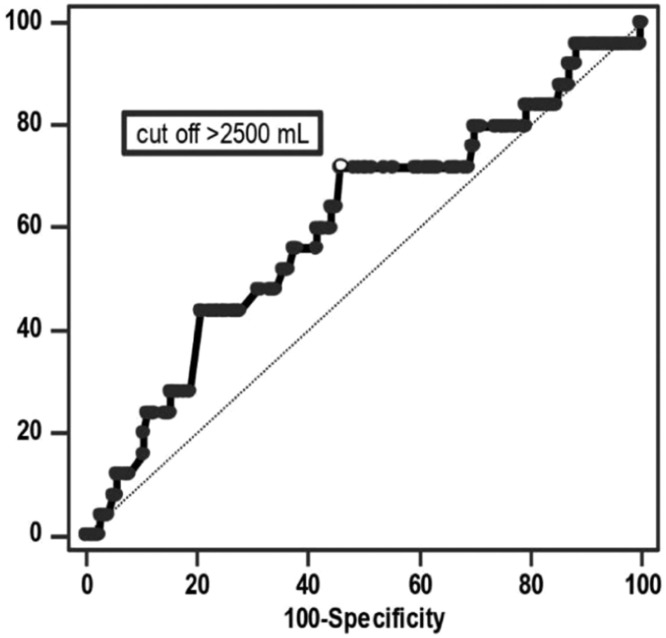
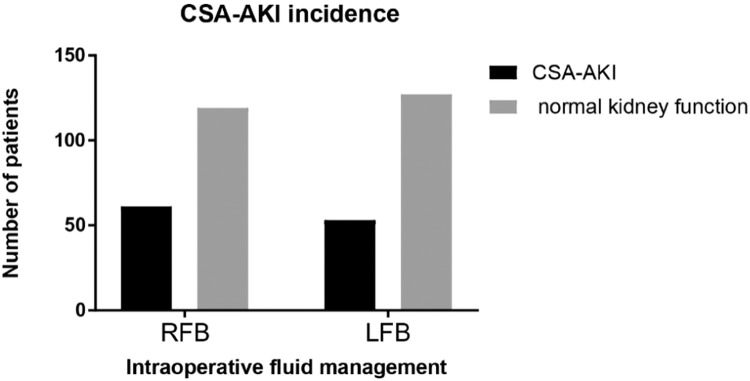
The primary endpoint was CSA-AKI. The secondary outcomes were in-hospital mortality, cardiovascular complications, ICU Length of Stay (ICU-LOS), and Hospital LOS (H-LOS). After propensity score matching, 180 patients remained in each group. There was no difference in risk of CSA-AKI between the two groups (RR = 1.15; 95% CI, 0.85-1.56, p = 0.36). The in-hospital mortality, H-LOS and cardiovascular complications were higher in the LFB group. ICU-LOS was not significantly different between the two groups. ROCcurve analysis determined a fluid balance above 2500 mL to accurately predict in-hospital mortality.
Patients undergoing on-pump CABG with LFB when compared with patients with RFB present similar CSA-AKI rates and ICU-LOS, but higher in-hospital mortality, cardiovascular complications, and H-LOS.
最近的数据表明,在接受大手术的患者中,术中液体治疗方案可能会影响患者的结局。非心脏手术中,术后急性肾损伤(AKI)的发生与限制性液体平衡(RFB)和自由性液体平衡(LFB)均相关。但在心脏手术患者中,这种影响尚不清楚。本研究的目的是评估术中 RFB 与 LFB 与心脏手术后 AKI(CSA-AKI)的发生率以及接受体外循环冠状动脉旁路移植术(CABG)的患者的主要术后结局之间的关系。
这是一项前瞻性、多中心、观察性队列研究,在巴西的两家高复杂性大学医院进行。择期接受体外循环 CABG 并需要术后重症监护的成年患者根据术中液体策略(RFB 或 LFB)分为两组,无干预措施。
主要终点是 CSA-AKI。次要结局是院内死亡率、心血管并发症、重症监护病房(ICU)住院时间(ICU-LOS)和医院住院时间(H-LOS)。在倾向评分匹配后,每组仍有 180 例患者。两组 CSA-AKI 的风险无差异(RR=1.15;95%CI,0.85-1.56,p=0.36)。LFB 组的院内死亡率、H-LOS 和心血管并发症更高,而 ICU-LOS 两组间无显著差异。ROC 曲线分析确定液体平衡超过 2500ml 可准确预测院内死亡率。
与 RFB 相比,接受体外循环 CABG 的患者采用 LFB 时,CSA-AKI 发生率和 ICU-LOS 相似,但院内死亡率、心血管并发症和 H-LOS 更高。