School of Public Health, University of Sydney, Sydney, Australia.
PLoS Med. 2010 Feb 23;7(2):e1000236. doi: 10.1371/journal.pmed.1000236.
Diabetes imposes a substantial burden globally in terms of premature mortality, morbidity, and health care costs. Estimates of economic outcomes associated with diabetes are essential inputs to policy analyses aimed at prevention and treatment of diabetes. Our objective was to estimate and compare event rates, hospital utilization, and costs associated with major diabetes-related complications in high-, middle-, and low-income countries.
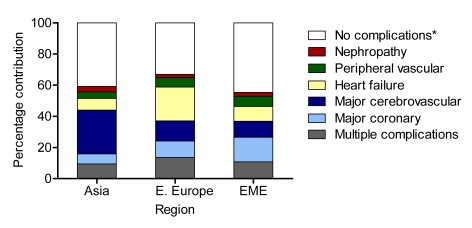
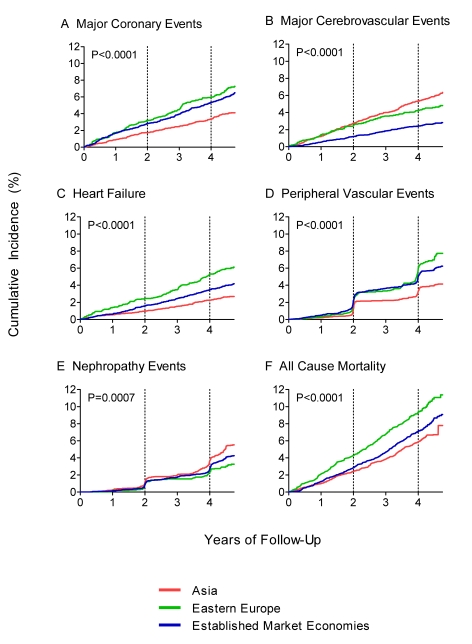
Incidence and history of diabetes-related complications, hospital admissions, and length of stay were recorded in 11,140 patients with type 2 diabetes participating in the Action in Diabetes and Vascular Disease (ADVANCE) study (mean age at entry 66 y). The probability of hospital utilization and number of days in hospital for major events associated with coronary disease, cerebrovascular disease, congestive heart failure, peripheral vascular disease, and nephropathy were estimated for three regions (Asia, Eastern Europe, and Established Market Economies) using multiple regression analysis. The resulting estimates of days spent in hospital were multiplied by regional estimates of the costs per hospital bed-day from the World Health Organization to compute annual acute and long-term costs associated with the different types of complications. To assist, comparability, costs are reported in international dollars (Int$), which represent a hypothetical currency that allows for the same quantities of goods or services to be purchased regardless of country, standardized on purchasing power in the United States. A cost calculator accompanying this paper enables the estimation of costs for individual countries and translation of these costs into local currency units. The probability of attending a hospital following an event was highest for heart failure (93%-96% across regions) and lowest for nephropathy (15%-26%). The average numbers of days in hospital given at least one admission were greatest for stroke (17-32 d across region) and heart failure (16-31 d) and lowest for nephropathy (12-23 d). Considering regional differences, probabilities of hospitalization were lowest in Asia and highest in Established Market Economies; on the other hand, lengths of stay were highest in Asia and lowest in Established Market Economies. Overall estimated annual hospital costs for patients with none of the specified events or event histories ranged from Int$76 in Asia to Int$296 in Established Market Economies. All complications included in this analysis led to significant increases in hospital costs; coronary events, cerebrovascular events, and heart failure were the most costly, at more than Int$1,800, Int$3,000, and Int$4,000 in Asia, Eastern Europe, and Established Market Economies, respectively.
Major complications of diabetes significantly increase hospital use and costs across various settings and are likely to impose a high economic burden on health care systems.
糖尿病在全球范围内导致了过早死亡、发病和医疗保健费用等方面的巨大负担。与糖尿病相关的经济结果的估计是旨在预防和治疗糖尿病的政策分析的重要投入。我们的目的是评估和比较高、中、低收入国家与主要糖尿病相关并发症相关的事件发生率、医院利用率和成本。
在参加糖尿病和血管疾病行动(ADVANCE)研究的 11140 名 2 型糖尿病患者中,记录了与糖尿病相关并发症、住院和住院时间的发病率和病史。使用多元回归分析,为三个地区(亚洲、东欧和发达市场经济体)估算了与冠心病、脑血管疾病、充血性心力衰竭、外周血管疾病和肾病相关的主要事件的住院利用率和住院天数。根据世界卫生组织的地区医院床位日成本估算,将住院天数乘以与不同类型并发症相关的年度急性和长期成本。为了便于比较,报告了以国际元(Int$)表示的成本,国际元是一种假设货币,允许在不考虑国家的情况下购买相同数量的商品或服务,以美国的购买力为标准。本文附带的成本计算器可用于估算个别国家的成本,并将这些成本转换为当地货币单位。在三个地区中,心力衰竭(93%-96%)后住院的概率最高,肾病(15%-26%)后住院的概率最低。至少有一次住院记录的住院天数最多的是中风(17-32 天,各地区)和心力衰竭(16-31 天),肾病(12-23 天)最短。考虑到区域差异,亚洲地区住院概率最低,发达市场经济体最高;另一方面,亚洲地区的住院时间最长,发达市场经济体最短。在没有指定事件或事件历史的情况下,每位患者的年度医院费用估计范围为亚洲的 76 国际元至发达市场经济体的 296 国际元。本分析中包括的所有并发症都导致了医院费用的显著增加;在亚洲、东欧和发达市场经济体中,冠心病事件、脑血管事件和心力衰竭的费用最高,分别超过 1800 国际元、3000 国际元和 4000 国际元。
糖尿病的主要并发症显著增加了各种情况下的医院使用和成本,并且很可能对医疗保健系统造成巨大的经济负担。