Urology Service, Department of Surgery, Sidney Kimmel Center for Prostate and Urologic Cancers, and Health Outcomes Research Group, New York, New York, USA.
J Urol. 2010 Apr;183(4):1366-72. doi: 10.1016/j.juro.2009.12.021. Epub 2010 Feb 25.
Enthusiasm for laparoscopic surgical approaches to prostate cancer treatment has grown despite limited evidence of improved outcomes compared with open radical prostatectomy. We compared laparoscopic prostatectomy with or without robotic assistance vs open radical prostatectomy in terms of postoperative outcomes and subsequent cancer directed therapy.
Using a population based cancer registry linked with Medicare claims we identified men 66 years old or older with localized prostate cancer who underwent radical prostatectomy from 2003 to 2005. Outcome measures were general medical/surgical complications and mortality within 90 days after surgery, genitourinary/bowel complications within 365 days, radiation therapy and/or androgen deprivation therapy within 365 days and length of hospital stay.
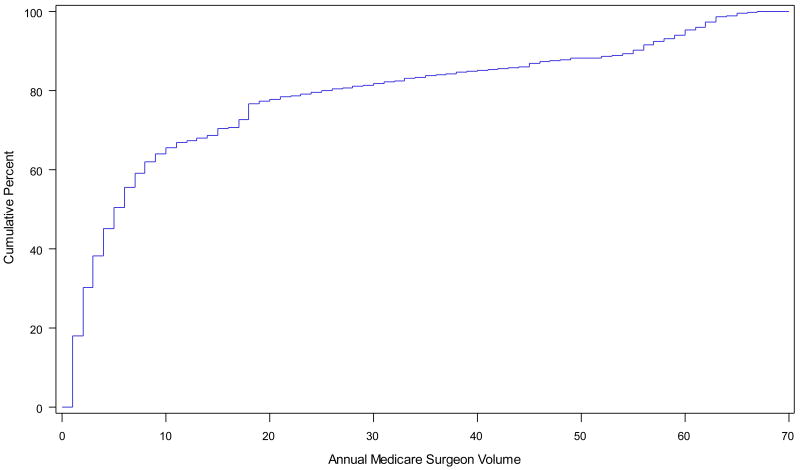
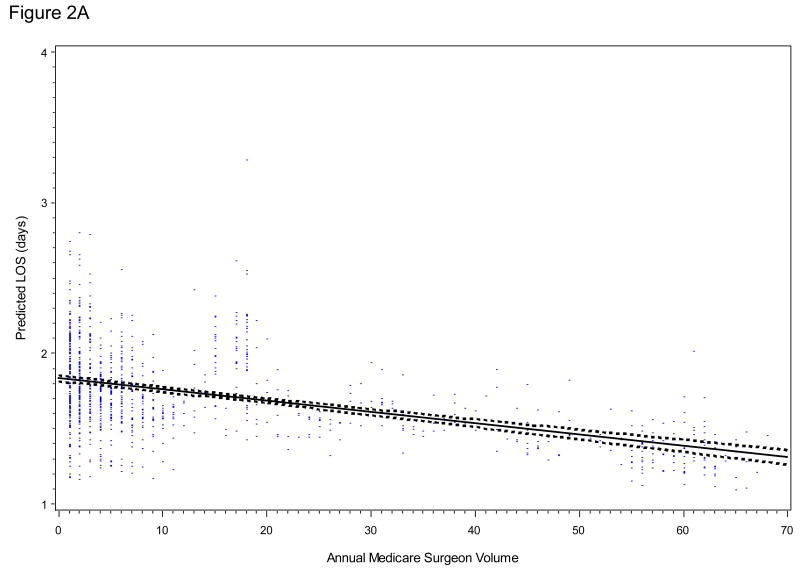
Of the 5,923 men 18% underwent laparoscopic radical prostatectomy. Adjusting for patient and tumor characteristics, there were no differences in the rate of general medical/surgical complications (OR 0.93 95% CI 0.77-1.14) or genitourinary/bowel complications (OR 0.96 95% CI 0.76-1.22), or in postoperative radiation and/or androgen deprivation (OR 0.80 95% CI 0.60-1.08). Laparoscopic prostatectomy was associated with a 35% shorter hospital stay (p <0.0001) and a lower bladder neck/urethral obstruction rate (OR 0.74, 95% CI 0.58-0.94). In laparoscopic cases surgeon volume was inversely associated with hospital stay and the odds of any genitourinary/bowel complication.
Laparoscopic prostatectomy and open radical prostatectomy have similar rates of postoperative morbidity and additional treatment. Men considering prostate cancer surgery should understand the expected benefits and risks of each technique to facilitate decision making and set realistic expectations.
尽管与开放性根治性前列腺切除术相比,腹腔镜前列腺癌治疗方法的疗效改善证据有限,但人们对其的热情依然高涨。我们比较了腹腔镜前列腺切除术联合或不联合机器人辅助手术与开放性根治性前列腺切除术在术后结果和随后的癌症定向治疗方面的差异。
我们利用基于人群的癌症登记系统和医疗保险索赔数据,确定了 2003 年至 2005 年间接受根治性前列腺切除术的年龄在 66 岁及以上的局限性前列腺癌患者。主要的观察指标包括术后 90 天内的一般医疗/手术并发症和死亡率、365 天内的泌尿/肠道并发症、365 天内的放疗和/或雄激素剥夺治疗以及住院时间。
在 5923 名男性患者中,18%接受了腹腔镜根治性前列腺切除术。调整患者和肿瘤特征后,一般医疗/手术并发症的发生率无差异(OR 0.93,95%CI 0.77-1.14)或泌尿/肠道并发症的发生率(OR 0.96,95%CI 0.76-1.22),或术后放疗和/或雄激素剥夺治疗的发生率(OR 0.80,95%CI 0.60-1.08)。腹腔镜前列腺切除术与住院时间缩短 35%(p<0.0001)和膀胱颈/尿道梗阻发生率降低(OR 0.74,95%CI 0.58-0.94)相关。在腹腔镜手术中,术者的手术量与住院时间和泌尿/肠道并发症的发生率呈负相关。
腹腔镜前列腺切除术和开放性根治性前列腺切除术的术后发病率和额外治疗的发生率相似。考虑接受前列腺癌手术的患者应了解每种技术的预期获益和风险,以便做出决策并设定合理的预期。