Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Welch Center for Prevention, Epidemiology, and Clinical Research, Baltimore, MD 21287, USA.
Am J Kidney Dis. 2010 Apr;55(4):648-59. doi: 10.1053/j.ajkd.2009.12.016. Epub 2010 Feb 26.
The Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) recently published an equation for estimated glomerular filtration rate (eGFR) using the same variables (serum creatinine level, age, sex, and race) as the Modification of Diet in Renal Disease (MDRD) Study equation. Although the CKD-EPI equation estimates GFR more precisely compared with the MDRD Study equation, whether this equation improves risk prediction is unknown.
Prospective cohort study, the Atherosclerosis Risk in Communities (ARIC) Study.
SETTING & PARTICIPANTS: 13,905 middle-aged participants without a history of cardiovascular disease with median follow-up of 16.9 years.
eGFR.
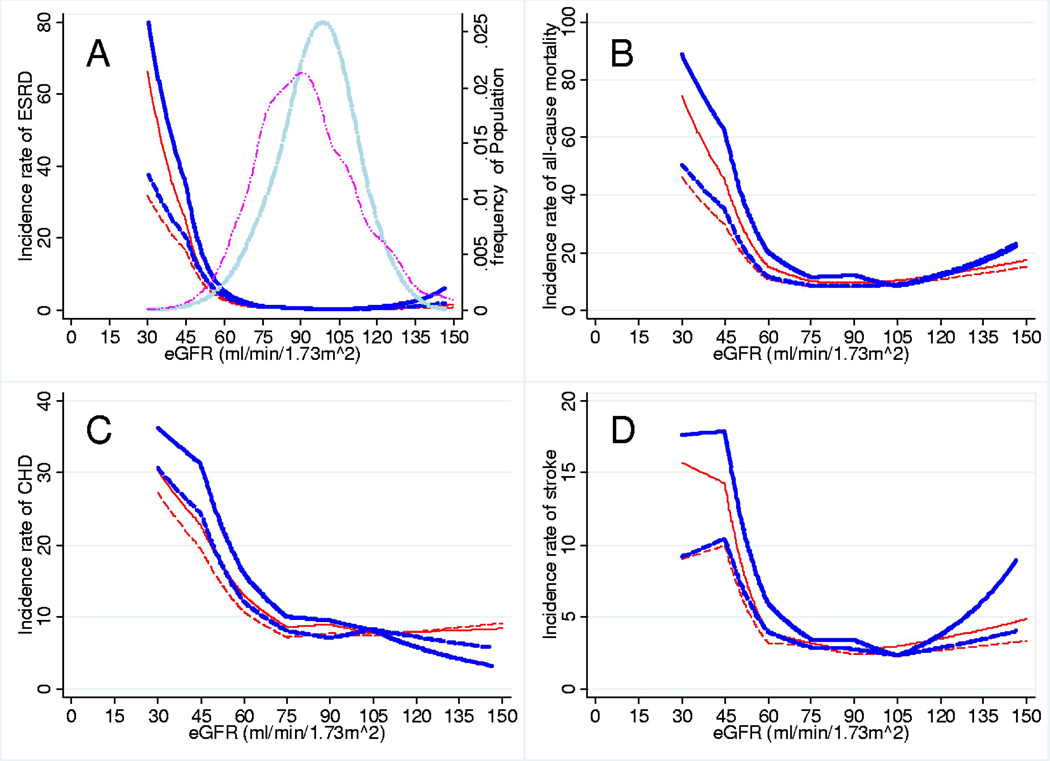
OUTCOMES & MEASUREMENTS: We compared the association of eGFR in categories (>or=120, 90-119, 60-89, 30-59, and <30 mL/min/1.73 m(2)) using the CKD-EPI and MDRD Study equations with risk of incident end-stage renal disease, all-cause mortality, coronary heart disease, and stroke.
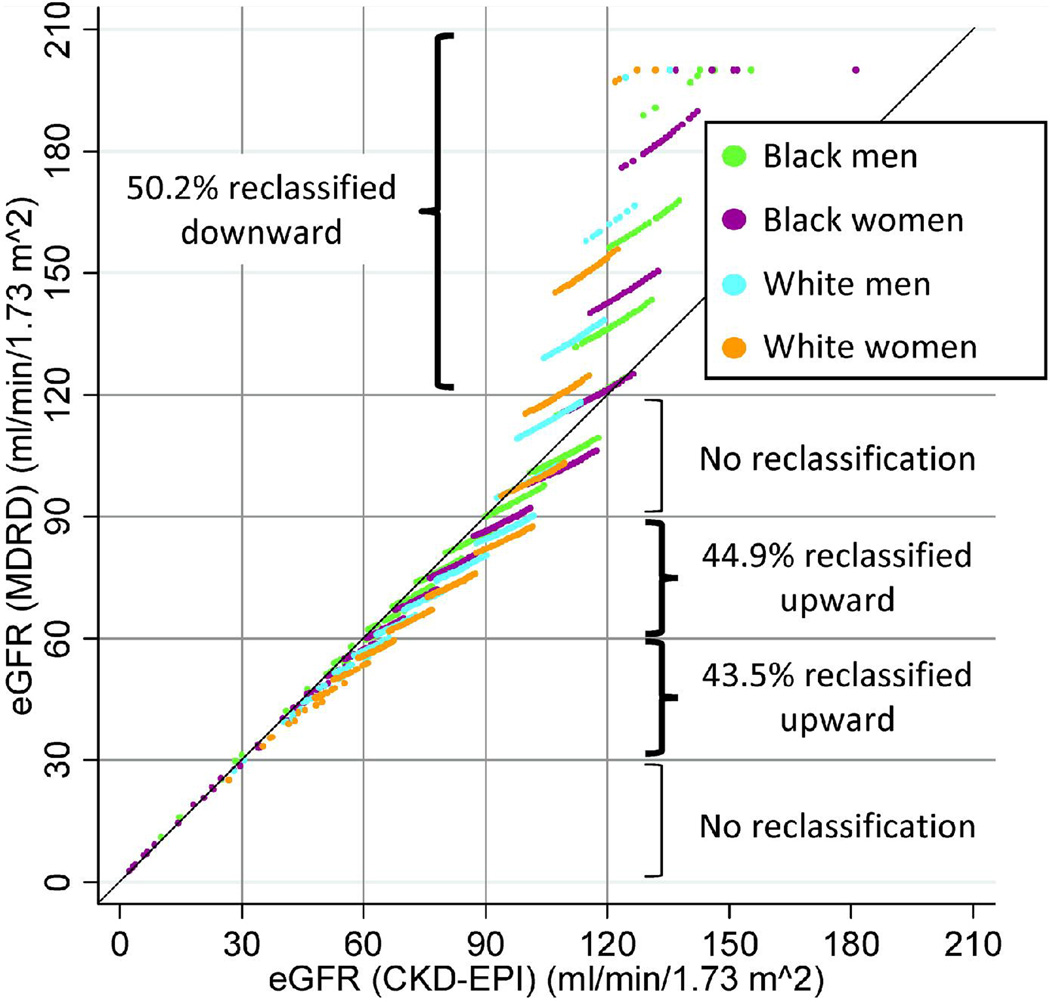
The median value for eGFR(CKD-EPI) was higher than that for eGFR(MDRD) (97.6 vs 88.8 mL/min/1.73 m(2); P < 0.001). The CKD-EPI equation reclassified 44.9% (n = 3,079) and 43.5% (n = 151) of participants with eGFR(MDRD) of 60-89 and 30-59 mL/min/1.73 m(2), respectively, upward to a higher eGFR category, but reclassified no one with eGFR(MDRD) of 90-119 or <30 mL/min/1.73 m(2), decreasing the prevalence of CKD stages 3-5 from 2.7% to 1.6%. Participants with eGFR(MDRD) of 30-59 mL/min/1.73 m(2) who were reclassified upward had lower risk compared with those who were not reclassified (end-stage renal disease incidence rate ratio, 0.10 [95% CI, 0.03-0.33]; all-cause mortality, 0.30 [95% CI, 0.19-0.48]; coronary heart disease, 0.36 [95% CI, 0.21-0.61]; and stroke, 0.50 [95% CI, 0.24-1.02]). Similar results were observed for participants with eGFR(MDRD) of 60-89 mL/min/1.73 m(2). More frequent reclassification of younger, female, and white participants explained some of these trends. Net reclassification improvement in participants with eGFR < 120 mL/min/1.73 m(2) was positive for all outcomes (P < 0.001).
Limited number of cases with eGFR < 60 mL/min/1.73 m(2) and no measurement of albuminuria.
The CKD-EPI equation more appropriately categorized individuals with respect to long-term clinical risk compared with the MDRD Study equation, suggesting improved clinical usefulness in this middle-aged population.
慢性肾脏病流行病学协作组(CKD-EPI)最近发布了一个基于血清肌酐水平、年龄、性别和种族等变量的肾小球滤过率(eGFR)估算公式,与肾脏病饮食改良研究(MDRD)方程相同。虽然 CKD-EPI 方程比 MDRD 研究方程更精确地估计 GFR,但该方程是否能改善风险预测尚不清楚。
前瞻性队列研究,即社区动脉粥样硬化风险研究(ARIC)。
13905 名无心血管疾病病史的中年参与者,中位随访时间为 16.9 年。
eGFR。
使用 CKD-EPI 和 MDRD 研究方程,我们比较了 eGFR 类别(>或=120、90-119、60-89、30-59 和<30 mL/min/1.73 m2)与终末期肾病、全因死亡率、冠心病和中风的风险之间的关联。
与 MDRD 研究方程相比,CKD-EPI 方程更适当地对长期临床风险进行分类,这表明该方程在该中年人群中有更好的临床应用价值。
eGFR < 60 mL/min/1.73 m2 的病例数量有限,且未测量白蛋白尿。