Brenner Bluma G, Coutsinos Dimitrios
McGill AIDS Centre, Lady Davis Institute, 3755 Cote Ste. Catherine Road, Montreal, Quebec, H3T 1E2, Canada.
HIV Ther. 2009 Nov 1;3(6):583-594. doi: 10.2217/hiv.09.40.
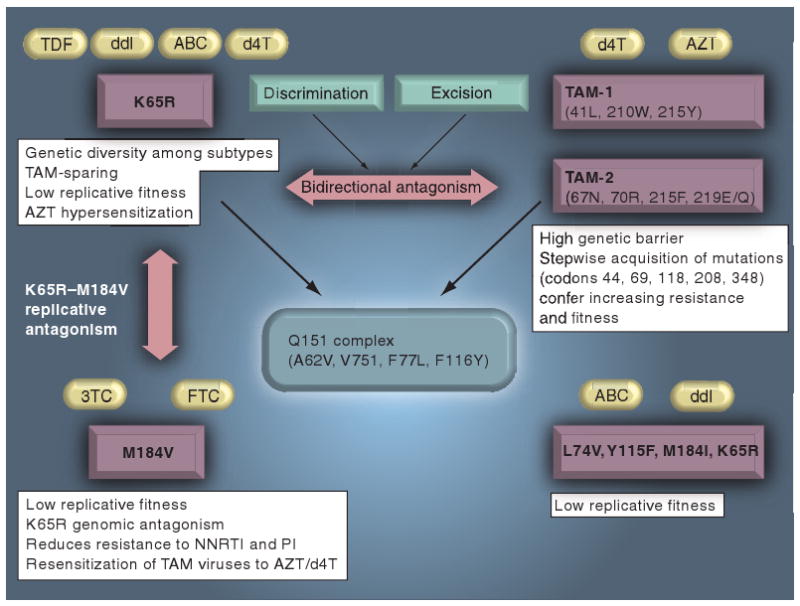
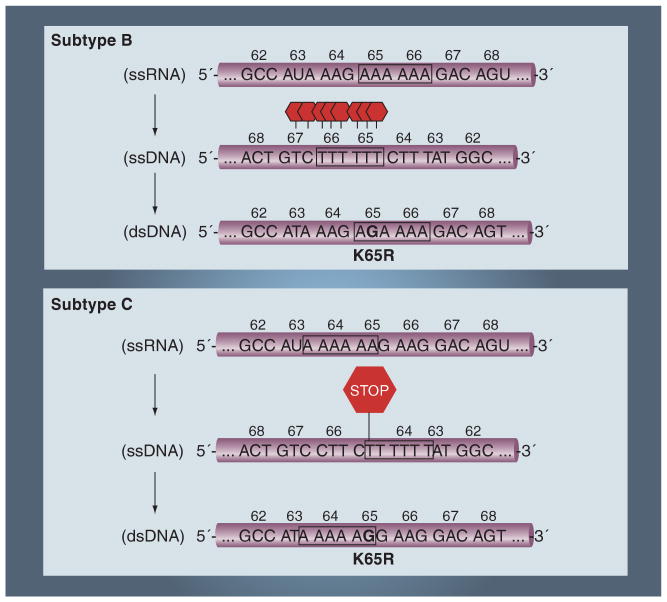
Resistance to antiviral therapy is the limiting factor in the successful management of HIV. In general, the K65R mutation is rarely selected (1.7-4%) with tenofovir disoproxil fumarate (TDF), abacavir (ABC), didanosine (ddI), and stavudine (d4T), as compared with the high incidence (>40%) of thymidine analog mutations associated with zidovudine and d4T. The high barrier to the development of K65R may reflect a combination of factors, including the high potency of K65R-selecting drugs, including recommended TDF/emtricitabine and ABC/lamivudine (ABC/3TC) combinations; the partial (low-intermediate level) profile of cross-resistance conferred by K65R to TDF, ABC and 3TC; the favorable viral fitness constraint imposed by K65R and the 3TC/emtricitabine-associated M184V mutations; the bidirectional antagonism between the K65R and thymidine analog mutation pathways; and unique RNA structural considerations in the region surrounding codon 65. Nevertheless, surprisingly high levels of treatment failures and K65R resistance may be associated with triple nucleoside analog regimens. The use of TDF + ABC, TDF + ddI and ABC + d4T in combination with 3TC or emtricitabine should be avoided. This selection of K65R may be reduced by the inclusion of zidovudine in two-four nucleoside reverse-transcriptase regimens. Clinical studies have demonstrated an increased frequency of K65R in association with suboptimal d4T and ddI regimens, as well as nevirapine and its resistance mutations Y181C and G190A. The potential for the development of the K65R mutation in subtype C is particularly problematic wherein a signature KKK nucleotide motif, at codons 64, 65 and 66 in reverse transcriptase, appear to lead to template pausing, facilitating the selection of K65R. Optimizing regimens may attenuate the emergence of K65R, leading to better long-term treatment management in different geographic settings. TDF-based regimens are the leading candidates for first- and second-line therapy, microbicides and chemoprophylaxis strategies.
对抗病毒治疗产生耐药性是成功管理HIV的限制因素。一般来说,与齐多夫定和司他夫定相关的胸苷类似物突变的高发生率(>40%)相比,替诺福韦酯(TDF)、阿巴卡韦(ABC)、去羟肌苷(ddI)和司他夫定(d4T)很少选择K65R突变(1.7 - 4%)。K65R突变产生的高屏障可能反映了多种因素的综合作用,包括选择K65R的药物的高效性,如推荐的TDF/恩曲他滨和ABC/拉米夫定(ABC/3TC)组合;K65R对TDF、ABC和3TC产生的部分(低 - 中等水平)交叉耐药性;K65R以及3TC/恩曲他滨相关的M184V突变所施加的有利的病毒适应性限制;K65R与胸苷类似物突变途径之间的双向拮抗作用;以及密码子65周围区域独特的RNA结构因素。然而,令人惊讶的是,高比例的治疗失败和K65R耐药性可能与三联核苷类似物方案有关。应避免将TDF + ABC、TDF + ddI和ABC + d4T与3TC或恩曲他滨联合使用。在二 - 四种核苷逆转录酶方案中加入齐多夫定可能会降低K65R的选择。临床研究表明,与次优的d4T和ddI方案以及奈韦拉平及其耐药突变Y181C和G190A相关的K65R频率增加。C亚型中K65R突变发生的可能性尤其成问题,其中逆转录酶中密码子64、65和66处的特征性KKK核苷酸基序似乎会导致模板停顿,并促进K65R的选择。优化方案可能会减弱K65R的出现,从而在不同地理环境中实现更好的长期治疗管理。基于TDF的方案是一线和二线治疗、杀微生物剂和化学预防策略的主要候选方案。