Institut de Recherche pour le Développement, University Montpellier 1, UMR 145, Montpellier, France.
BMC Public Health. 2010 Mar 1;10:105. doi: 10.1186/1471-2458-10-105.
Coinfection with hepatitis B virus (HBV) or hepatitis C virus (HCV) in HIV-infected patients receiving a commonly used nevirapine-based antiretroviral therapy is a major concern for African clinicians owing to its high prevalence, the infrequent testing and treatment of viral hepatitis, and the impact of liver disease on the tolerability and effectiveness of anti-HIV treatment. We compared the hepatotoxicity and the immunological, virological and clinical effectiveness of a nevirapine-based antiretroviral therapy between patients infected with HIV only and patients coinfected with hepatitis B or C virus in Cameroon.
A retrospective cohort study was conducted among HIV-1-infected patients. Plasma HBV DNA and HCV RNA were tested in positive or indeterminate samples for HBsAg or HCV antibodies, respectively. All patients received nevirapine and lamivudine plus stavudine or zidovudine.
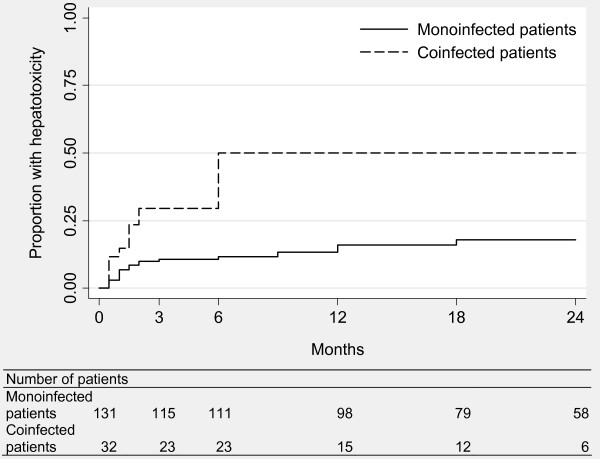
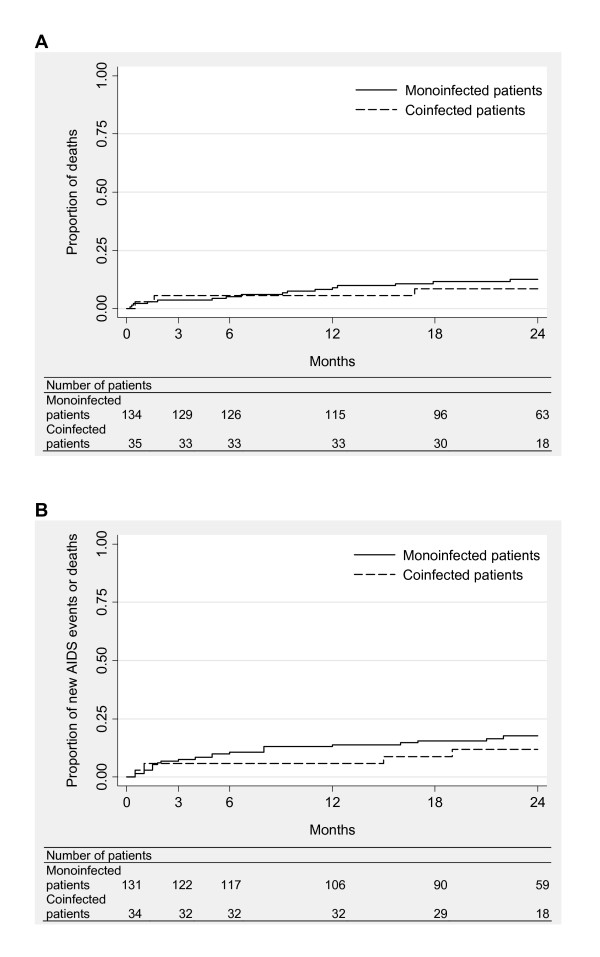
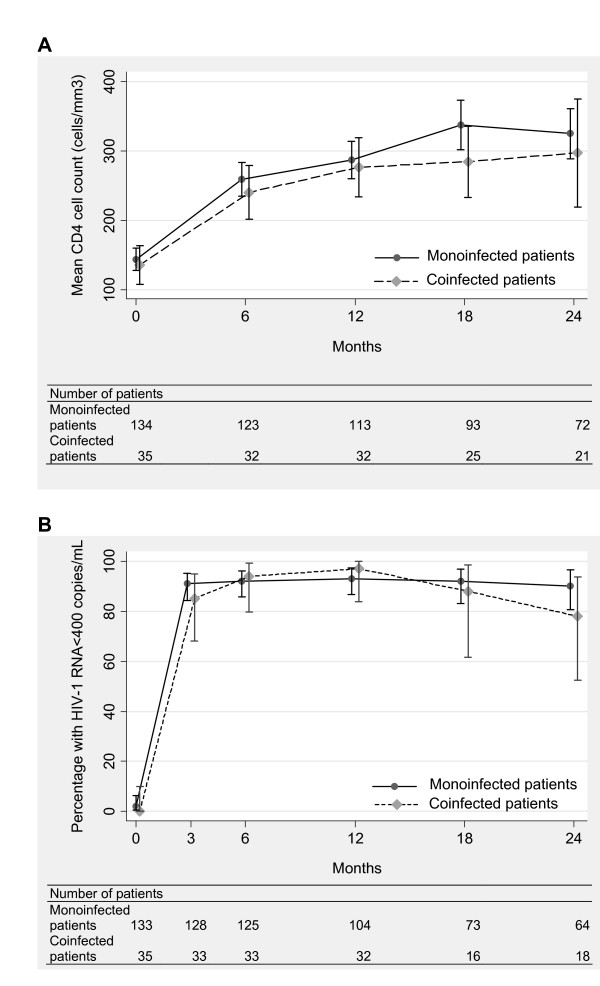
Of 169 HIV-1-infected patients with a median baseline CD4 count of 135 cells/mm3 (interquartile range [IQR] 67-218), 21% were coinfected with HBV or HCV. In coinfected patients, the median viral load was 2.47 x 107 IU/mL for HBV (IQR 3680-1.59 x 108) and 928 000 IU/mL for HCV (IQR 178 400-2.06 x 106). Multivariate analyses showed that the risk of hepatotoxicity was 2-fold higher in coinfected patients (p < 0.01). The response to antiretroviral therapy was however comparable between monoinfected and coinfected patients in terms of CD4 cell count increase (p = 0.8), HIV-1 viral load below 400 copies/mL (p = 0.9), death (p = 0.3) and death or new AIDS-defining event (p = 0.1). Nevirapine was replaced by a protease inhibitor in 4 patients owing to hepatotoxicity.
This study suggests that the nevirapine-based antiretroviral therapy could be used safely as first-line treatment in patients with low CD4 cell count in Africa despite frequent coinfections with HBV or HCV and infrequent testing of these infections. Although testing for HBV and HCV should be systematically performed before initiating antiretroviral therapy, transaminases elevations at baseline or during treatment should be a decisive argument for testing when hepatitis status is unknown.
在接受常用的基于奈韦拉平的抗逆转录病毒疗法的 HIV 感染者中,乙型肝炎病毒(HBV)或丙型肝炎病毒(HCV)合并感染是非洲临床医生关注的一个主要问题,这是由于其高流行率、对病毒性肝炎的检测和治疗不频繁,以及肝脏疾病对抗 HIV 治疗的耐受性和有效性的影响。我们比较了喀麦隆感染 HIV 患者和合并感染乙型肝炎或丙型肝炎病毒患者的基于奈韦拉平的抗逆转录病毒治疗的肝毒性以及免疫、病毒学和临床疗效。
对 169 例 HIV-1 感染患者进行了回顾性队列研究。在 HBsAg 或 HCV 抗体阳性或不确定的样本中检测血浆 HBV DNA 和 HCV RNA。所有患者均接受奈韦拉平、拉米夫定加司他夫定或齐多夫定治疗。
在中位基线 CD4 计数为 135 个细胞/mm3(四分位间距 [IQR]67-218)的 169 例 HIV-1 感染患者中,21%合并感染 HBV 或 HCV。在合并感染患者中,HBV 的中位病毒载量为 2.47×107IU/mL(IQR3680-1.59×108),HCV 的中位病毒载量为 928000IU/mL(IQR178400-2.06×106)。多变量分析显示,合并感染患者发生肝毒性的风险增加了 2 倍(p<0.01)。然而,就 CD4 细胞计数增加(p=0.8)、HIV-1 病毒载量<400 拷贝/mL(p=0.9)、死亡(p=0.3)和死亡或新发 AIDS 定义性事件(p=0.1)而言,抗逆转录病毒治疗的反应在单感染和合并感染患者之间是可比的。由于肝毒性,有 4 例患者将奈韦拉平替换为蛋白酶抑制剂。
尽管经常合并感染 HBV 或 HCV,且这些感染的检测不频繁,但本研究表明,在非洲低 CD4 细胞计数患者中,基于奈韦拉平的抗逆转录病毒治疗可作为一线治疗安全使用。尽管应在开始抗逆转录病毒治疗前系统地检测 HBV 和 HCV,但在治疗期间或治疗前基线转氨酶升高应是检测肝炎状态未知的决定性依据。