Sanders Gillian D, Anaya Henry D, Asch Steven, Hoang Tuyen, Golden Joya F, Bayoumi Ahmed M, Owens Douglas K
Duke Clinical Research Institute, Duke University, PO Box 17969, Durham, NC 27715, USA.
J Gen Intern Med. 2010 Jun;25(6):556-63. doi: 10.1007/s11606-010-1265-5. Epub 2010 Mar 4.
The CDC recommends routine voluntary HIV testing of all patients 13-64 years of age. Despite this recommendation, HIV testing rates are low even among those at identifiable risk, and many patients do not return to receive their results.
To examine the costs and benefits of strategies to improve HIV testing and receipt of results.
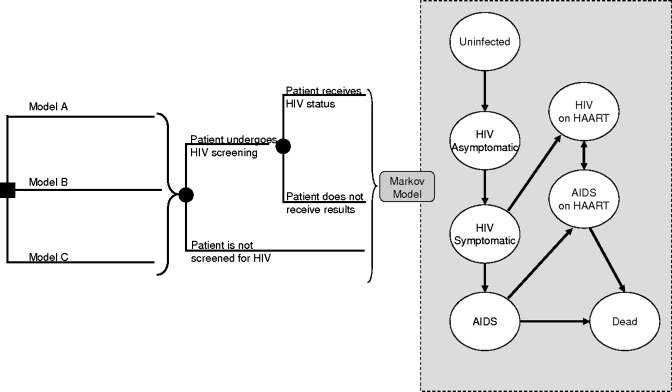
Cost-effectiveness analysis based on a Markov model. Acceptance of testing, return rates, and related costs were derived from a randomized trial of 251 patients; long-term costs and health outcomes were derived from the literature. SETTING/TARGET POPULATION: Primary-care patients with unknown HIV status.
Comparison of three intervention models for HIV counseling and testing: Model A = traditional HIV counseling and testing; Model B = nurse-initiated routine screening with traditional HIV testing and counseling; Model C = nurse-initiated routine screening with rapid HIV testing and streamlined counseling.
Life-years, quality-adjusted life-years (QALYs), costs and incremental cost-effectiveness.
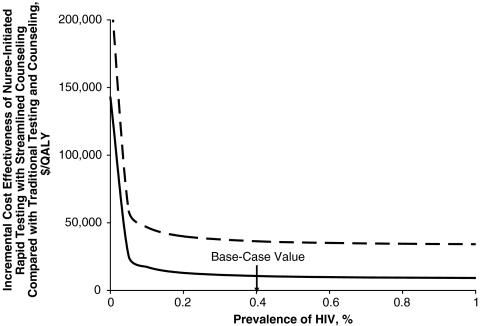
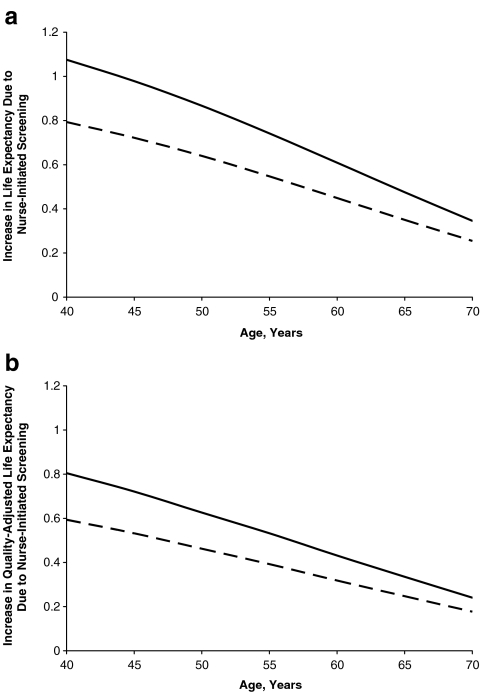
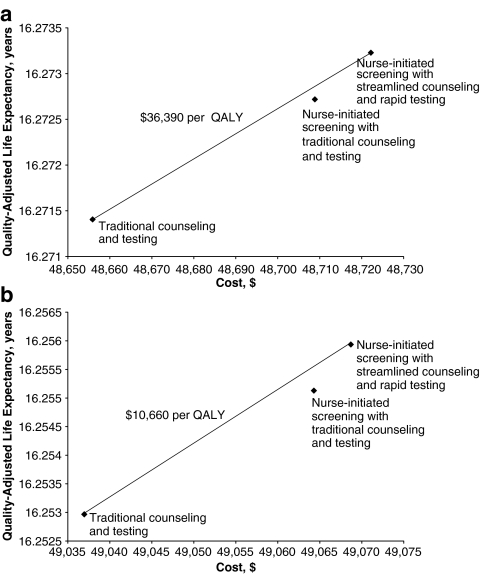
Without consideration of the benefit from reduced HIV transmission, Model A resulted in per-patient lifetime discounted costs of $48,650 and benefits of 16.271 QALYs. Model B increased lifetime costs by $53 and benefits by 0.0013 QALYs (corresponding to 0.48 quality-adjusted life days). Model C cost $66 more than Model A with an increase of 0.0018 QALYs (0.66 quality-adjusted life days) and an incremental cost-effectiveness of $36,390/QALY. When we included the benefit from reduced HIV transmission, Model C cost $10,660/QALY relative to Model A. The cost-effectiveness of Model C was robust in sensitivity analyses.
In a primary-care population, nurse-initiated routine screening with rapid HIV testing and streamlined counseling increased rates of testing and receipt of test results and was cost-effective compared with traditional HIV testing strategies.
美国疾病控制与预防中心建议对所有13至64岁的患者进行常规自愿性艾滋病毒检测。尽管有此建议,但即使在有明确风险的人群中,艾滋病毒检测率也很低,而且许多患者没有返回获取检测结果。
研究提高艾滋病毒检测及结果获取率策略的成本与效益。
基于马尔可夫模型的成本效益分析。检测接受率、返回率及相关成本来自对251名患者的一项随机试验;长期成本和健康结果来自文献。
设置/目标人群:艾滋病毒感染状况未知的初级保健患者。
比较三种艾滋病毒咨询与检测干预模式:模式A = 传统艾滋病毒咨询与检测;模式B = 护士发起的常规筛查及传统艾滋病毒检测与咨询;模式C = 护士发起的常规筛查及快速艾滋病毒检测与简化咨询。
生命年、质量调整生命年(QALY)、成本及增量成本效益。
在不考虑减少艾滋病毒传播带来的益处的情况下,模式A导致每位患者终身贴现成本为48,650美元,效益为16.271个QALY。模式B使终身成本增加53美元,效益增加0.0013个QALY(相当于0.48个质量调整生命日)。模式C比模式A成本高66美元,QALY增加0.0018个(0.66个质量调整生命日),增量成本效益为36,390美元/QALY。当我们纳入减少艾滋病毒传播带来的益处时,模式C相对于模式A的成本效益为10,660美元/QALY。在敏感性分析中,模式C的成本效益很稳健。
在初级保健人群中,护士发起的常规筛查及快速艾滋病毒检测与简化咨询提高了检测率和检测结果获取率,与传统艾滋病毒检测策略相比具有成本效益。