Harvard Combined Orthopaedic Residency Program, Department of Orthopaedic Surgery, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA.
J Orthop Surg Res. 2010 Jan 22;5:4. doi: 10.1186/1749-799X-5-4.
Femoral skeletal traction assists in the reduction and transient stabilization of pelvic, acetabular, hip, and femoral fractures when splinting is ineffective. Traditional teaching has recommended a medial entry site for insertion of the traction pin in order to minimize injury to the femoral artery as it passes through Hunter's canal. The present anatomical study evaluates the risk to the femoral artery and other medial neurovascular structures using a lateral entry approach.
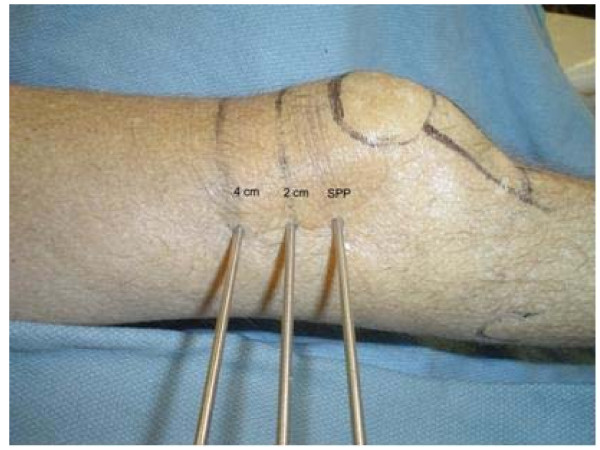
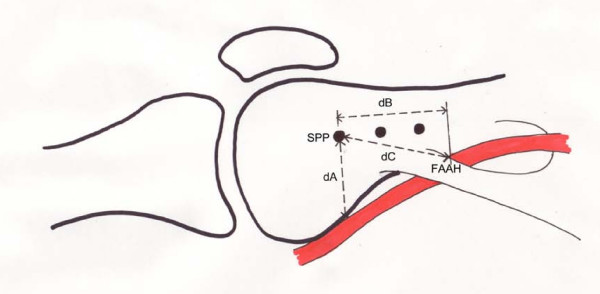
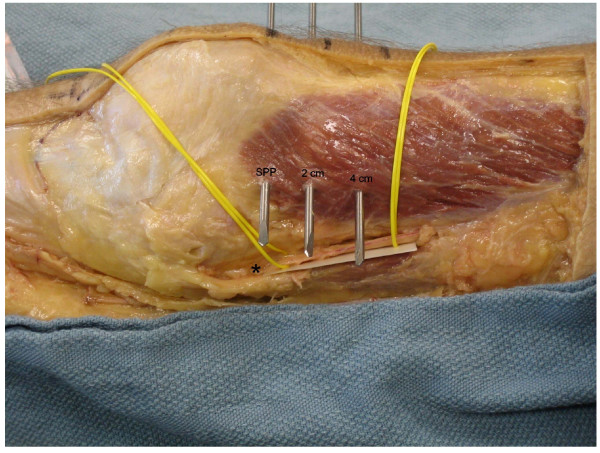
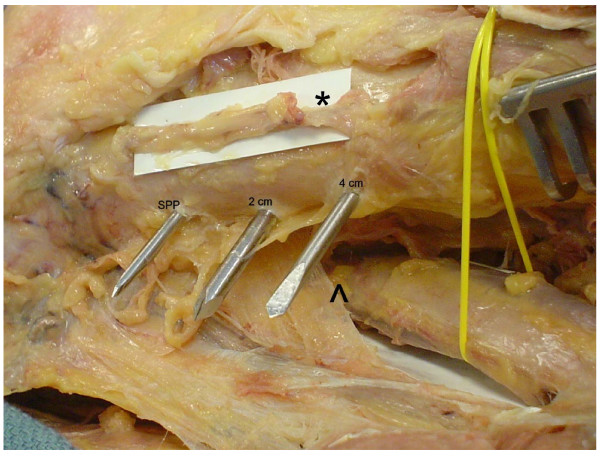
Six embalmed cadavers (twelve femurs) were obtained for dissection. Steinman pins were drilled from lateral to medial at the level of the superior pole of the patella, at 2 cm, and at 4 cm proximal to this point. Medial superficial dissection was then performed to identify the saphenous nerve, the superior medial geniculate artery, the adductor hiatus, the tendinous insertion of the adductor magnus and the femoral artery. Measurements localizing these anatomic structures relative to the pins were obtained.
The femoral artery was relatively safe and was no closer than 29.6 mm (mean) from any of the three Steinman pins. The superior medial geniculate artery was the medial structure at most risk.
Lateral femoral traction pin entry is a safe procedure with minimal risk to the saphenous nerve and femoral artery. Of the structures examined, only the superior medial geniculate artery is at a risk of iatrogenic injury due to its position. The incidence of such injury in clinical practice and its clinical significance is not known. Lateral insertion facilitates traction pin placement since it minimizes the need to move the contralateral extremity out of the way of the drilling equipment or the need to elevate or externally rotate the injured extremity relative to the contralateral extremity.
当夹板固定无效时,股骨骨骼牵引有助于骨盆、髋臼、髋部和股骨骨折的复位和暂时稳定。传统的教学方法推荐经内侧入路置入牵引针,以最大程度地减少股动脉在经过亨特管时的损伤。本解剖学研究使用外侧入路评估了牵引针插入时对股动脉和其他内侧神经血管结构的风险。
从六个防腐尸体(十二根股骨)中获得解剖标本。从髌骨上极水平、距髌骨上极 2cm 和 4cm 处,从外侧向内侧钻入史丹曼针。然后进行内侧浅层解剖,以识别隐神经、上内侧膝状动脉、收肌裂孔、大收肌腱止点和股动脉。测量这些解剖结构相对于针的定位。
股动脉相对安全,与三根史丹曼针的距离均不小于 29.6mm(平均值)。上内侧膝状动脉是最易受损伤的内侧结构。
外侧股骨牵引针入路是一种安全的操作,对隐神经和股动脉的风险最小。在所检查的结构中,只有上内侧膝状动脉由于其位置而有发生医源性损伤的风险。在临床实践中这种损伤的发生率及其临床意义尚不清楚。外侧插入便于牵引针的放置,因为它最大限度地减少了对钻孔设备的另一侧肢体的避让,或需要相对于对侧肢体抬高或外旋受伤肢体的需要。