The Department of Neurobiology and Anatomy, The University of Texas Medical School, Houston, Texas, USA.
J Neuroinflammation. 2010 Mar 11;7:19. doi: 10.1186/1742-2094-7-19.
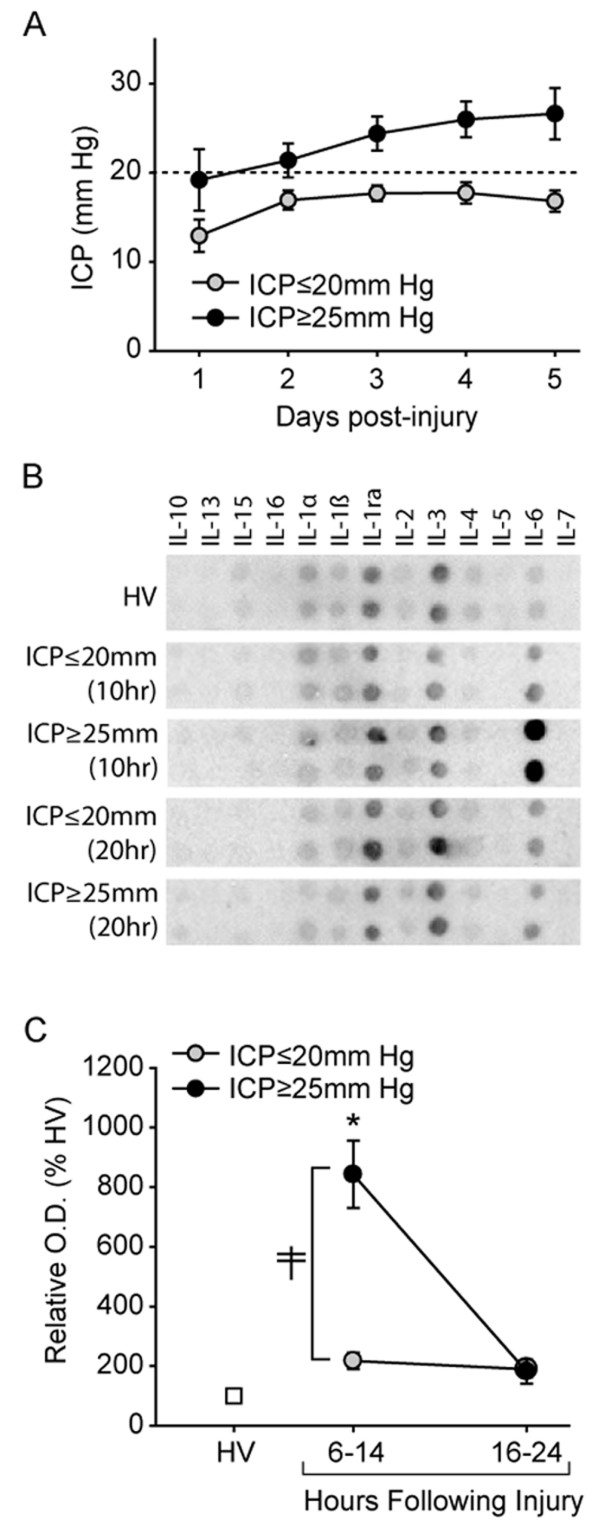
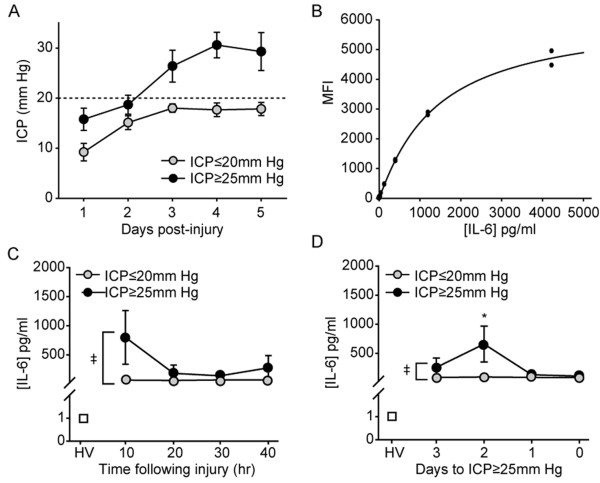
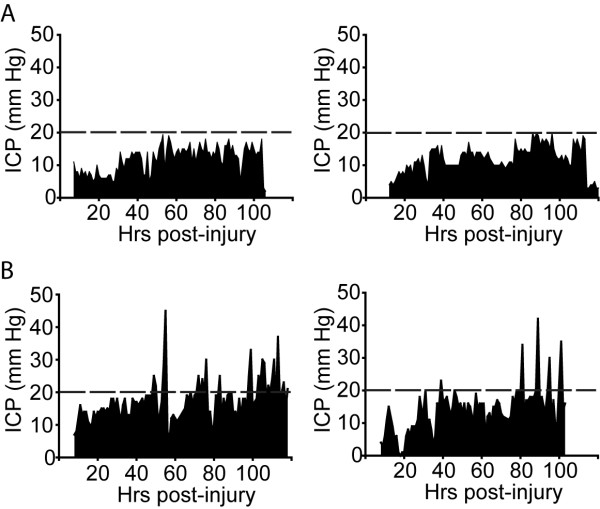
Increased intracranial pressure (ICP) is a serious, life-threatening, secondary event following traumatic brain injury (TBI). In many cases, ICP rises in a delayed fashion, reaching a maximal level 48-96 hours after the initial insult. While pressure catheters can be implanted to monitor ICP, there is no clinically proven method for determining a patient's risk for developing this pathology.
In the present study, we employed antibody array and Luminex-based screening methods to interrogate the levels of inflammatory cytokines in the serum of healthy volunteers and in severe TBI patients (GCS<or=8) with or without incidence of elevated intracranial pressure (ICP). De-identified samples and ELISAs were used to confirm the sensitivity and specificity of IL-6 as a prognostic marker of elevated ICP in both isolated TBI patients, and polytrauma patients with TBI.
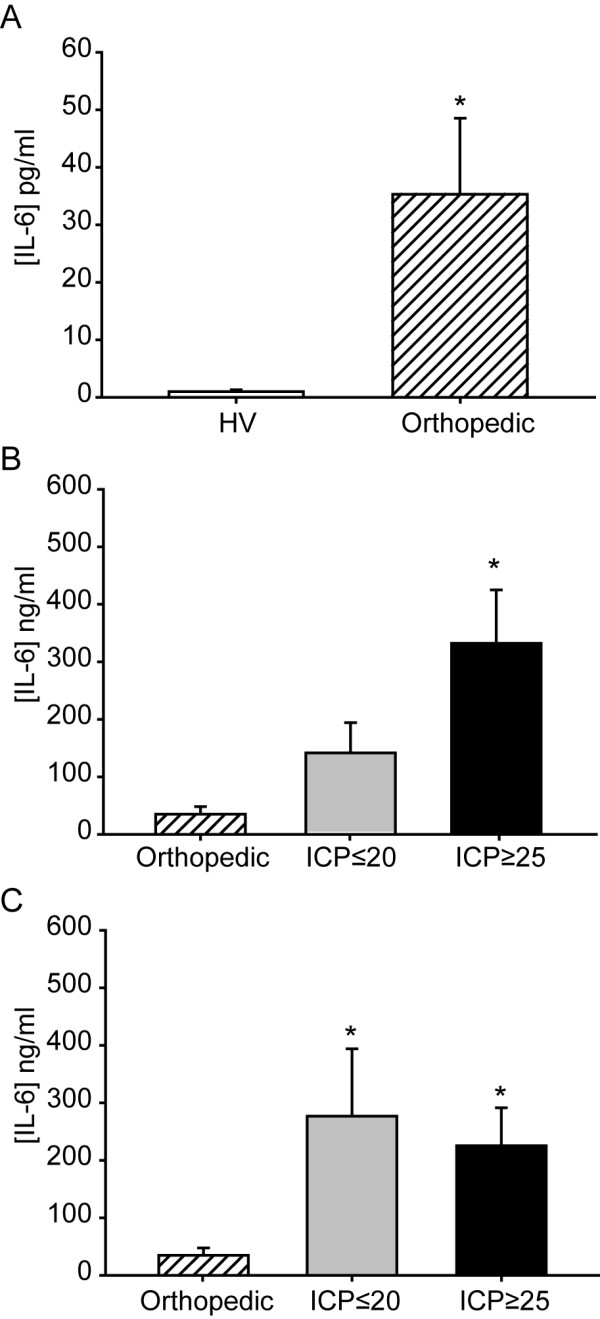
Consistent with previous reports, we observed sustained increases in IL-6 levels in TBI patients irrespective of their ICP status. However, the group of patients who subsequently experienced ICP >or= 25 mm Hg had significantly higher IL-6 levels within the first 17 hours of injury as compared to the patients whose ICP remained <or=20 mm Hg. When blinded samples (n = 22) were assessed, a serum IL-6 cut-off of <5 pg/ml correctly identified 100% of all the healthy volunteers, a cut-off of >128 pg/ml correctly identified 85% of isolated TBI patients who subsequently developed elevated ICP, and values between these cut-off values correctly identified 75% of all patients whose ICP remained <or=20 mm Hg throughout the study period. In contrast, the marker had no prognostic value in predicting elevated ICP in polytrauma patients with TBI. When the levels of serum IL-6 were assessed in patients with orthopedic injury (n = 7) in the absence of TBI, a significant increase was found in these patients compared to healthy volunteers, albeit lower than that observed in TBI patients.
Our results suggest that serum IL-6 can be used for the differential diagnosis of elevated ICP in isolated TBI.
颅内压(ICP)升高是颅脑损伤(TBI)后的一种严重的、危及生命的继发性疾病。在许多情况下,ICP 呈延迟性升高,在初始损伤后 48-96 小时达到最高水平。虽然可以植入压力导管来监测 ICP,但目前还没有临床证实的方法来确定患者发生这种病理的风险。
在本研究中,我们采用抗体阵列和基于 Luminex 的筛选方法,检测健康志愿者和伴有或不伴有颅内压升高(ICP)的严重 TBI 患者(GCS<或=8)的血清中炎症细胞因子的水平。使用去识别样本和 ELISA 来确认 IL-6 作为 TBI 患者 ICP 升高的预后标志物的敏感性和特异性,包括单纯 TBI 患者和合并 TBI 的多发创伤患者。
与之前的报告一致,我们观察到 TBI 患者的 IL-6 水平持续升高,无论其 ICP 状态如何。然而,随后发生 ICP>或=25mmHg 的患者在损伤后的前 17 小时内的 IL-6 水平明显更高,而 ICP 保持<或=20mmHg 的患者则没有。当对盲样(n=22)进行评估时,血清 IL-6 截断值<5pg/ml 正确识别了 100%的所有健康志愿者,截断值>128pg/ml 正确识别了 85%的随后发生 ICP 升高的单纯 TBI 患者,而在这些截断值之间的患者则正确识别了所有 ICP 在整个研究期间保持<或=20mmHg 的患者的 75%。相比之下,该标志物在预测合并 TBI 的多发创伤患者的 ICP 升高方面没有预测价值。当评估无 TBI 的骨科损伤患者(n=7)的血清 IL-6 水平时,与健康志愿者相比,这些患者的 IL-6 水平显著升高,尽管低于 TBI 患者。
我们的结果表明,血清 IL-6 可用于鉴别诊断单纯 TBI 患者的 ICP 升高。