Department of Nephrology and Medical Intensive Care Medicine, Charité Universitätsmedizin Berlin, Campus Virchow-Klinikum, Augustenburgerplatz 1, Berlin, Germany.
Crit Care. 2010;14(2):R69. doi: 10.1186/cc8975. Epub 2010 Apr 19.
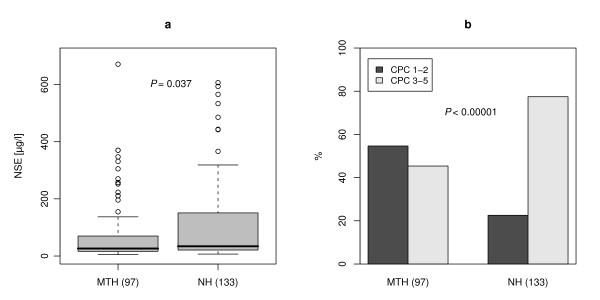
Neuron specific enolase (NSE) has been proven effective in predicting neurological outcome after cardiac arrest with a current cut off recommendation of 33 microg/l. However, most of the corresponding studies were conducted before the introduction of mild therapeutic hypothermia (MTH). Therefore we conducted a study investigating the association between NSE and neurological outcome in patients treated with MTH.
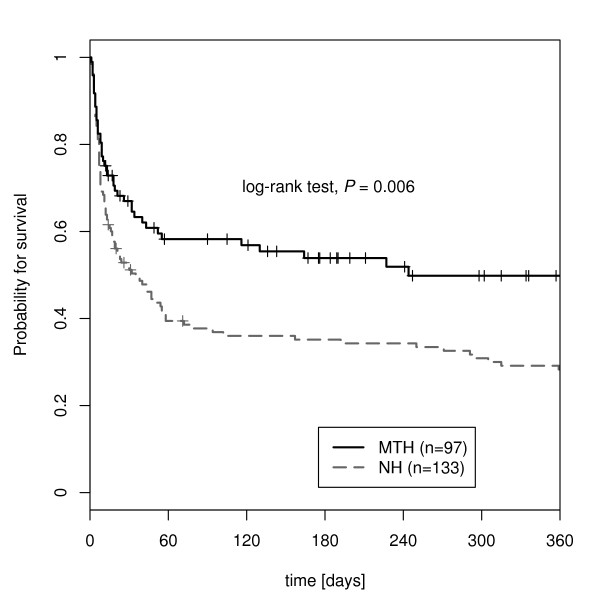
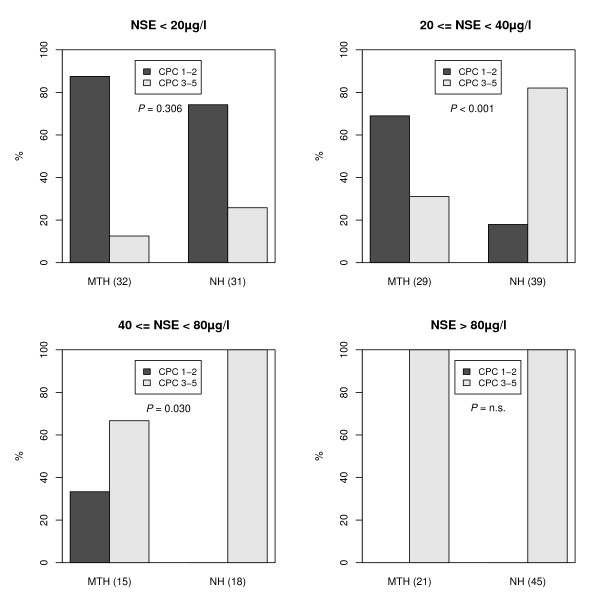
In this prospective observational cohort study the data of patients after cardiac arrest receiving MTH (n = 97) were consecutively collected and compared with a retrospective non-hypothermia (NH) group (n = 133). Serum NSE was measured 72 hours after admission to ICU. Neurological outcome was classified according to the Pittsburgh cerebral performance category (CPC 1 to 5) at ICU discharge.
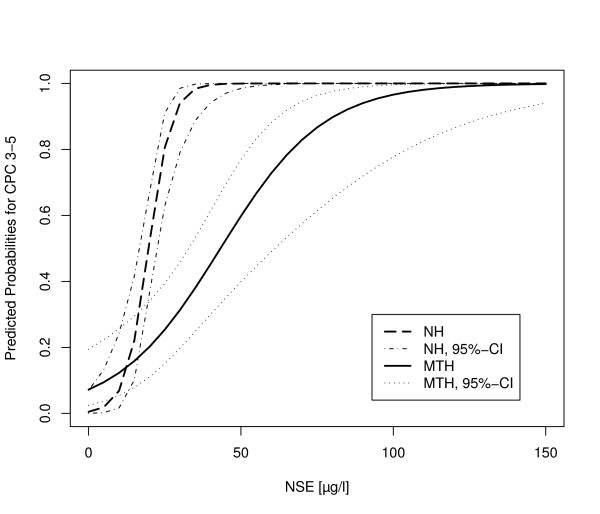
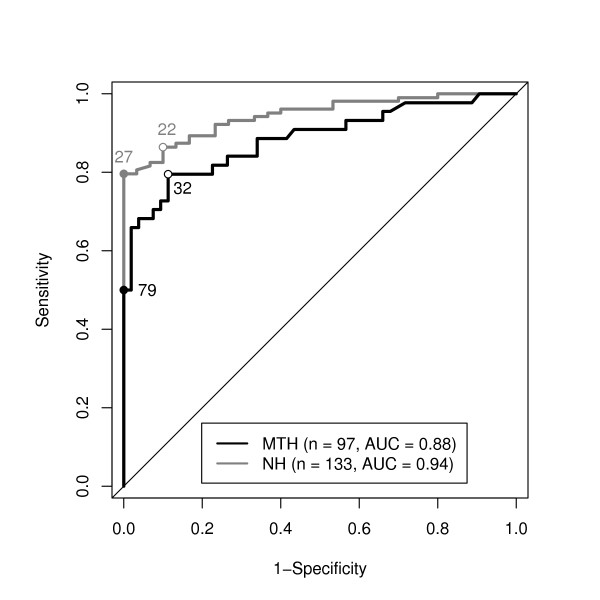
NSE serum levels were significantly lower under MTH compared to NH in univariate analysis. However, in a linear regression model NSE was affected significantly by time to return of spontaneous circulation (ROSC) and ventricular fibrillation rhythm but not by MTH. The model for neurological outcome identified NSE, NSE*MTH (interaction) as well as time to ROSC as significant predictors. Receiver Operating Characteristic (ROC) analysis revealed a higher cutoff value for unfavourable outcome (CPC 3 to 5) with a specificity of 100% in the hypothermia group (78.9 microg/l) compared to the NH group (26.9 microg/l).
Recommended cutoff levels for NSE 72 hours after ROSC do not reliably predict poor neurological outcome in cardiac arrest patients treated with MTH. Prospective multicentre trials are required to re-evaluate NSE cutoff values for the prediction of neurological outcome in patients treated with MTH.
神经元特异性烯醇化酶(NSE)已被证明可有效预测心脏骤停后的神经功能预后,目前推荐的截断值为 33μg/l。然而,大多数相关研究都是在轻度治疗性低体温(MTH)引入之前进行的。因此,我们进行了一项研究,调查了接受 MTH 治疗的患者中 NSE 与神经功能预后之间的关系。
在这项前瞻性观察性队列研究中,连续收集了接受 MTH 治疗的心脏骤停患者(n=97)的数据,并与回顾性非低体温(NH)组(n=133)进行了比较。入院后 72 小时测量血清 NSE。神经功能预后根据 ICU 出院时的匹兹堡脑功能分类(CPC 1-5)进行分类。
在单变量分析中,MTH 组的 NSE 血清水平明显低于 NH 组。然而,在线性回归模型中,NSE 受自主循环恢复(ROSC)时间和室颤节律的影响显著,但不受 MTH 的影响。神经功能预后模型确定了 NSE、NSE*MTH(交互作用)以及 ROSC 时间作为显著的预测因子。接受者操作特征(ROC)分析显示,低温组(78.9μg/l)NSE 截断值对于不良预后(CPC 3-5)的特异性为 100%,高于 NH 组(26.9μg/l)。
推荐的 ROSC 后 72 小时 NSE 截断值不能可靠地预测接受 MTH 治疗的心脏骤停患者的不良神经功能预后。需要进行前瞻性多中心试验,以重新评估接受 MTH 治疗的患者中 NSE 截断值预测神经功能预后的效果。