Department of Primary Health Care, University of Oxford, Oxford, UK.
BMC Cardiovasc Disord. 2010 Apr 19;10:18. doi: 10.1186/1471-2261-10-18.
Selection of the right warfarin dose at the outset of treatment is not straightforward, and current evidence is lacking to determine the optimal strategy for initiation of therapy.
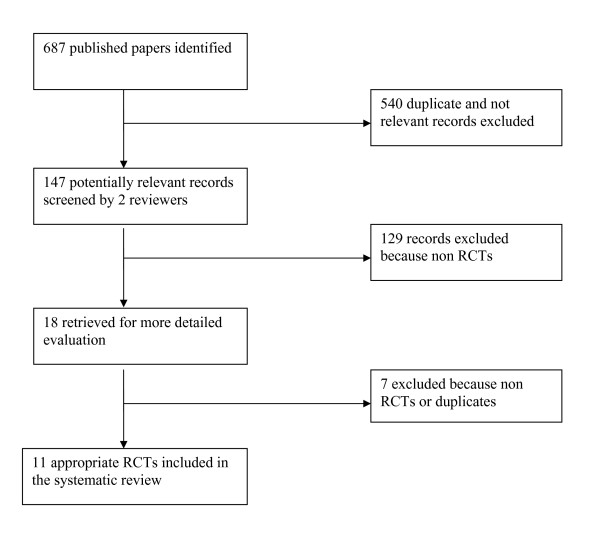
We included randomized controlled trials in patients commencing anticoagulation with warfarin, comparing different loading dose or different regimens.We searched Medline, EMBASE, the Cochrane Library and the NHS Health Economics Database up to June 2009. Primary outcomes were time to stable INR and adverse events. We summarised results as proportion of INRs in range from date of initiation and compared dichotomous outcomes using relative risks (RR) and calculated 95% confidence intervals (CIs).
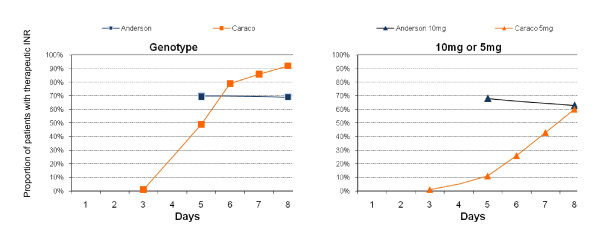
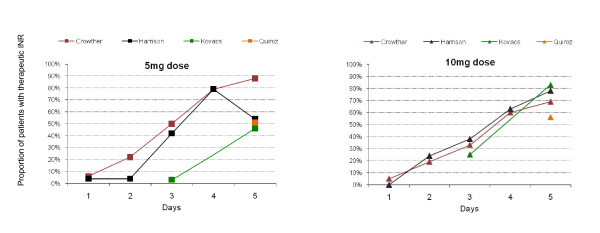
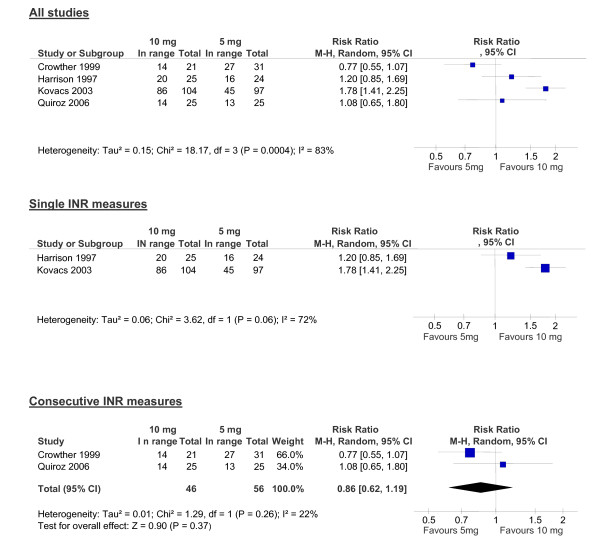
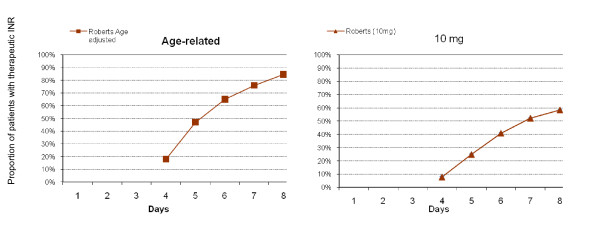
We included 11 studies of 1,340 patients newly initiated on warfarin. In two studies that used single INR measures, a loading dose of 10 mg compared to 5 mg led to more patients in range on day five. However, in two studies which measured two consecutive INRs, a loading dose of 10 mg compared to 5 mg did not lead to more patients in range on day five (RR = 0.86, 95% CI, 0.62 to 1.19, p = 0.37). Patients receiving a 2.5 mg initiation does took longer to achieve the therapeutic range, whilst those receiving a calculated initiation dose achieved target range 0.8 days quicker (4.2 days vs. 5 days, p = 0.007). More elderly patients receiving an age adjusted dose achieved a stable INR compared to the Fennerty protocol (48% vs. 22% p = 0.02) and significantly fewer patients on the age adjusted regimens had high out-of-range INRs. Two studies report no significant differences between genotype guided and 5 mg or 10 mg initiation doses and in the one significant genotype study the control group INRs were significantly lower than expected.
Our review findings suggest there is still considerable uncertainty between a 10 mg and a 5 mg loading dose for initiation of warfarin. In the elderly, lower initiation doses or age adjusted doses are more appropriate, leading to less higher INRs. Currently there is insufficient evidence to warrant genotype guided initiation, and adequately powered trials to detect effects on adverse events are currently warranted.
在治疗开始时选择合适的华法林剂量并不简单,目前缺乏确定治疗起始最佳策略的证据。
我们纳入了开始用华法林抗凝治疗的患者的随机对照试验,比较了不同的负荷剂量或不同的方案。我们检索了 Medline、EMBASE、Cochrane 图书馆和 NHS 健康经济学数据库,检索时间截至 2009 年 6 月。主要结局是稳定 INR 时间和不良事件。我们总结了起始日期后 INRs 范围内的比例,并使用相对危险度(RR)比较二分类结局,并计算了 95%置信区间(CI)。
我们纳入了 11 项共 1340 例新开始用华法林治疗的患者的研究。在两项使用单次 INR 测量的研究中,与 5mg 相比,10mg 负荷剂量导致第 5 天更多的患者在范围内。然而,在两项连续测量两次 INR 的研究中,与 5mg 相比,10mg 负荷剂量并未导致第 5 天更多的患者在范围内(RR = 0.86,95%CI,0.62 至 1.19,p = 0.37)。接受 2.5mg 起始剂量的患者达到治疗范围所需的时间较长,而接受计算得出的起始剂量的患者达到目标范围的时间快 0.8 天(4.2 天比 5 天,p = 0.007)。接受年龄调整剂量的老年患者达到稳定 INR 的比例高于 Fennerty 方案(48%比 22%,p = 0.02),并且接受年龄调整方案的患者中高 OUT-OF-RANGE INR 的比例显著较低。两项研究报告基因型指导与 5mg 或 10mg 起始剂量之间没有显著差异,在一项有意义的基因型研究中,对照组的 INR 明显低于预期。
我们的综述结果表明,华法林起始时 10mg 和 5mg 负荷剂量之间仍存在相当大的不确定性。在老年人中,较低的起始剂量或年龄调整剂量更为合适,导致较高 INR 的比例较低。目前,没有足够的证据支持基因型指导的起始,目前需要进行足够大的、能检测到不良事件影响的试验。