Centre for Infectious Disease Control, National Institute for Public Health and the Environment, Bilthoven, The Netherlands.
PLoS One. 2010 Apr 29;5(4):e10406. doi: 10.1371/journal.pone.0010406.
Although syndromic surveillance is increasingly used to detect unusual illness, there is a debate whether it is useful for detecting local outbreaks. We evaluated whether syndromic surveillance detects local outbreaks of lower-respiratory infections (LRIs) without swamping true signals by false alarms.
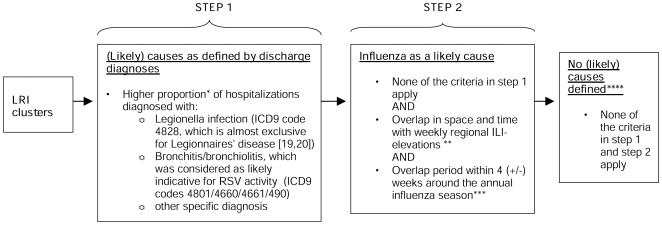
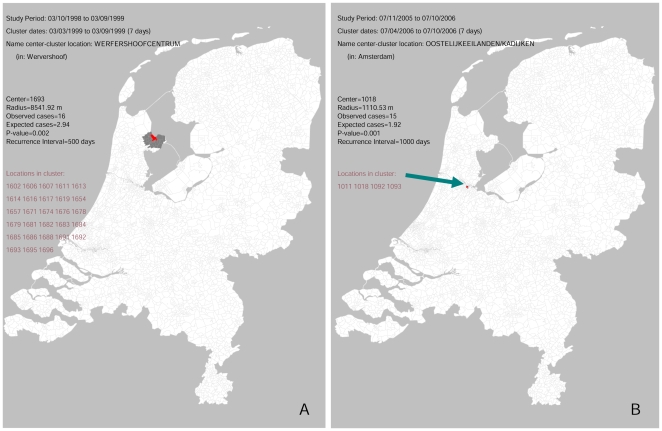
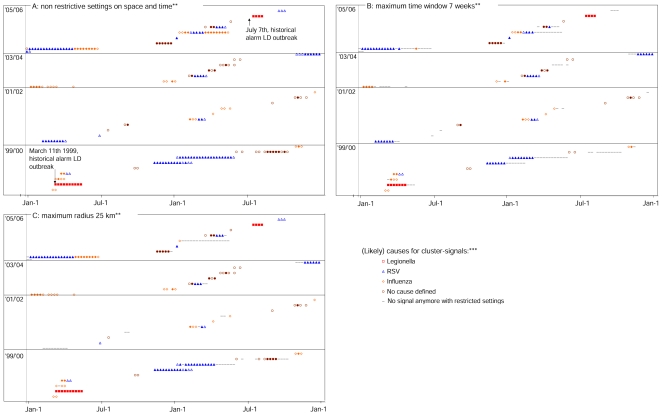
Using retrospective hospitalization data, we simulated prospective surveillance for LRI-elevations. Between 1999-2006, a total of 290762 LRIs were included by date of hospitalization and patients place of residence (>80% coverage, 16 million population). Two large outbreaks of Legionnaires disease in the Netherlands were used as positive controls to test whether these outbreaks could have been detected as local LRI elevations. We used a space-time permutation scan statistic to detect LRI clusters. We evaluated how many LRI-clusters were detected in 1999-2006 and assessed likely causes for the cluster-signals by looking for significantly higher proportions of specific hospital discharge diagnoses (e.g. Legionnaires disease) and overlap with regional influenza elevations. We also evaluated whether the number of space-time signals can be reduced by restricting the scan statistic in space or time. In 1999-2006 the scan-statistic detected 35 local LRI clusters, representing on average 5 clusters per year. The known Legionnaires' disease outbreaks in 1999 and 2006 were detected as LRI-clusters, since cluster-signals were generated with an increased proportion of Legionnaires disease patients (p:<0.0001). 21 other clusters coincided with local influenza and/or respiratory syncytial virus activity, and 1 cluster appeared to be a data artifact. For 11 clusters no likely cause was defined, some possibly representing as yet undetected LRI-outbreaks. With restrictions on time and spatial windows the scan statistic still detected the Legionnaires' disease outbreaks, without loss of timeliness and with less signals generated in time (up to 42% decline).
To our knowledge this is the first study that systematically evaluates the performance of space-time syndromic surveillance with nationwide high coverage data over a longer period. The results show that syndromic surveillance can detect local LRI-outbreaks in a timely manner, independent of laboratory-based outbreak detection. Furthermore, since comparatively few new clusters per year were observed that would prompt investigation, syndromic hospital-surveillance could be a valuable tool for detection of local LRI-outbreaks.
虽然症候群监测越来越多地用于检测异常疾病,但对于其是否有助于检测局部疫情仍存在争议。我们评估了症候群监测是否能够在不被虚假警报淹没真实信号的情况下检测到下呼吸道感染(LRIs)的局部疫情。
使用回顾性住院数据,我们模拟了前瞻性的 LRI 升高监测。1999-2006 年期间,根据住院日期和患者居住地(覆盖 80%以上人群,1600 万人口)纳入了 290762 例 LRI。荷兰两次军团病大暴发被用作阳性对照,以测试这些暴发是否可以被检测为局部 LRI 升高。我们使用时空置换扫描统计来检测 LRI 集群。我们评估了 1999-2006 年期间检测到多少个 LRI 集群,并通过寻找特定医院出院诊断(如军团病)的比例显著升高以及与区域流感升高的重叠,来评估集群信号的可能原因。我们还评估了通过限制扫描统计的空间或时间是否可以减少时空信号的数量。在 1999-2006 年期间,扫描统计检测到 35 个局部 LRI 集群,平均每年 5 个集群。1999 年和 2006 年已知的军团病暴发被检测为 LRI 集群,因为集群信号是由军团病患者比例增加而产生的(p:<0.0001)。21 个其他集群与当地流感和/或呼吸道合胞病毒活动相吻合,1 个集群似乎是数据异常。对于 11 个集群,没有明确的原因,其中一些可能代表尚未检测到的 LRI 暴发。在限制时间和空间窗口的情况下,扫描统计仍然检测到军团病暴发,没有失去及时性,并且在时间上生成的信号更少(减少高达 42%)。
据我们所知,这是第一项使用全国性高覆盖率数据在较长时间内系统评估时空症候群监测性能的研究。结果表明,症候群监测可以及时检测到局部 LRI 暴发,独立于基于实验室的暴发检测。此外,由于每年观察到的新集群相对较少,这将促使进行调查,因此,医院症候群监测可能是检测局部 LRI 暴发的有价值工具。