Moi University School of Medicine, Eldoret, Kenya.
Trop Med Int Health. 2010 Jul;15(7):833-41. doi: 10.1111/j.1365-3156.2010.02539.x. Epub 2010 May 14.
To describe incidence rates (IR) and risk factors for loss-to-follow-up (LTFU) among HIV-infected and HIV-exposed children in a large HIV treatment programme in Western Kenya.
The USAID-AMPATH Partnership has enrolled >100,000 patients (20% children) at 23 clinic sites throughout western Kenya. LTFU is defined as being absent from the clinic for >3 months if on combination antiretroviral treatment (cART) and >6 months if not. Included in this analysis were children aged <14 years, HIV exposed or infected at enrollment, and enrolled between April 2002 and March 2009. The IR for LTFU are presented per 100 child-years (CY) of follow-up. Proportional hazards models with time-independent and time-dependent covariates were used to model factors associated with LTFU. Weight for height Z-scores were calculated using EpiInfo, with severe malnutrition being defined as a Z-score <or=-3.0. Immune suppression was defined as per WHO age-specific categories.
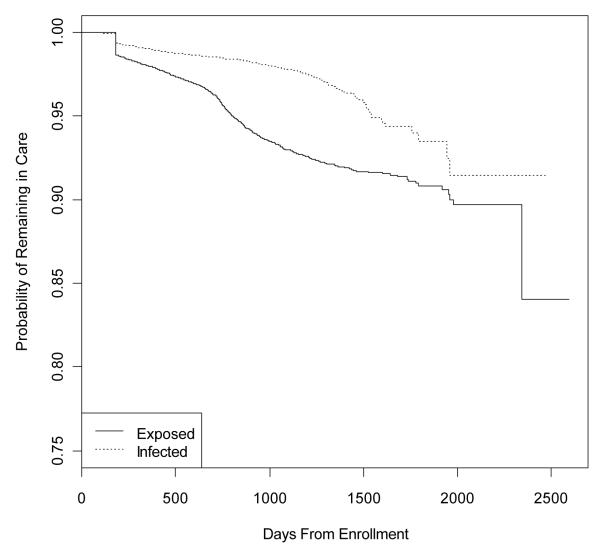
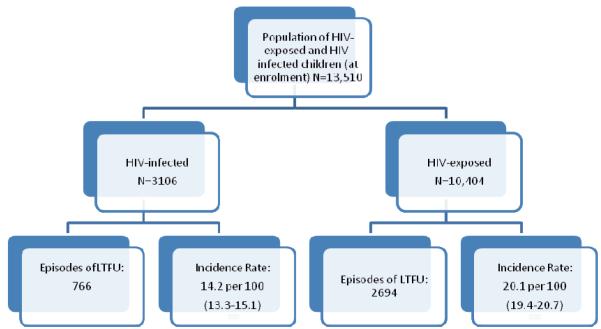
There were 13,510 children eligible for analysis, comprising 3106 children who at enrollment were HIV infected and 10,404 children who were HIV exposed. The overall IR of LTFU was 18.4 (17.8-18.9) per 100 CY. Among HIV-infected children, 15.2 (13.8-16.7) and 14.1 (13.1-15.8) per 100 CY became LTFU, pre- and post-cART initiation, respectively. The only independent risk factor for becoming LTFU among the HIV-infected children was severe immune suppression (AHR: 2.17, 95% CI: 1.51-3.12). Among the HIV-exposed children, 20.1 per 100 (19.4-20.7) became LTFU. Independent risk factors for LTFU among them were being severely low weight for height (AHR: 1.69, 95% CI: 1.25-2.28), being orphaned at enrollment (AHR: 1.57, 95% CI: 1.23-1.64), being CDC Class B or C (AHR: 1.41, 95% CI: 1.14-1.74), and having received cART (AHR: 1.56, 95% CI: 1.23-1.99). Protective against becoming LTFU among the HIV exposed were testing HIV positive (AHR: 0.26, 95% CI: 0.21-0.32), older age (AHR: 0.90, 95% CI: 0.85-0.96), enrolling in later time periods, and receiving food supplementation (AHR: 0.58, 95% CI: 0.32-1.04).
There is a high rate of LTFU among these highly vulnerable children, particularly among the HIV exposed. These data suggest that HIV-infected and HIV-exposed children are at especially high risk for LTFU if they are sick or malnourished.
描述在肯尼亚西部一个大型艾滋病毒治疗项目中,艾滋病毒感染和艾滋病毒暴露儿童的失访率(LTFU)的发生率(IR)和危险因素。
美国国际开发署 AMPATH 伙伴关系已经在肯尼亚西部的 23 个诊所招募了超过 100,000 名患者(20%为儿童)。如果正在接受联合抗逆转录病毒治疗(cART),则将 LTFU 定义为在诊所外超过 3 个月,如果未接受 cART,则超过 6 个月。本分析包括年龄<14 岁的儿童、入组时 HIV 感染或暴露的儿童,以及 2002 年 4 月至 2009 年 3 月期间入组的儿童。LTFU 的发生率以每 100 个儿童年(CY)的随访时间表示。采用具有时间独立和时间依赖协变量的比例风险模型来评估与 LTFU 相关的因素。使用 EpiInfo 计算体重身高 Z 评分,严重营养不良定义为 Z 评分<或=-3.0。免疫抑制定义为按照世卫组织年龄特定类别。
共有 13510 名符合分析条件的儿童,其中 3106 名儿童入组时 HIV 感染,10404 名儿童 HIV 暴露。LTFU 的总体发生率为 18.4(17.8-18.9)/100 CY。在 HIV 感染儿童中,分别在 cART 启动前和启动后,有 15.2(13.8-16.7)和 14.1(13.1-15.8)/100 CY 的儿童成为 LTFU。HIV 感染儿童成为 LTFU 的唯一独立危险因素是严重免疫抑制(AHR:2.17,95%CI:1.51-3.12)。在 HIV 暴露儿童中,有 20.1/100(19.4-20.7)成为 LTFU。LTFU 的独立危险因素包括严重低体重身高(AHR:1.69,95%CI:1.25-2.28)、入组时为孤儿(AHR:1.57,95%CI:1.23-1.64)、CDC 分类 B 或 C(AHR:1.41,95%CI:1.14-1.74)以及接受 cART(AHR:1.56,95%CI:1.23-1.99)。对于 HIV 暴露儿童,HIV 检测呈阳性(AHR:0.26,95%CI:0.21-0.32)、年龄较大(AHR:0.90,95%CI:0.85-0.96)、较晚时间入组和接受食物补充(AHR:0.58,95%CI:0.32-1.04)可预防成为 LTFU。
这些高度脆弱的儿童失访率很高,特别是在 HIV 暴露的儿童中。这些数据表明,如果 HIV 感染和 HIV 暴露的儿童生病或营养不良,他们特别容易失访。