Murillo Anays, DeSilva Mary Bachman, Sabin Lora L, Halim Nafisa, Chemusto Harriet, Aroda Philip, Gasuza Julia, Hamer Davidson H, Williams Anna Larson, Mukasa Barbara, Messersmith Lisa J, Bonawitz Rachael
Department of Global Health, Boston University School of Public Health, Boston University, 801 Massachusetts Avenue Crosstown Center, 3 Floor, Boston, MA, 02118 USA.
University of New England, 716 Stevens Ave, Portland, ME, 04103 USA.
Int J MCH AIDS. 2020;9(3):320-329. doi: 10.21106/ijma.380. Epub 2020 Jul 29.
Uganda has successfully reduced pediatric HIV infections through prevention of mother-to-child transmission of HIV (PMTCT) programs, yet little is known about adherence to infant-specific components of interventions. We hypothesized that infants born to mothers receiving the WiseMama (WM) electronic drug monitoring (EDM)-based adherence intervention would have increased uptake of six-week post-natal nevirapine (NVP) infant prophylaxis and better adherence to six-week early infant diagnosis (EID) HIV testing.
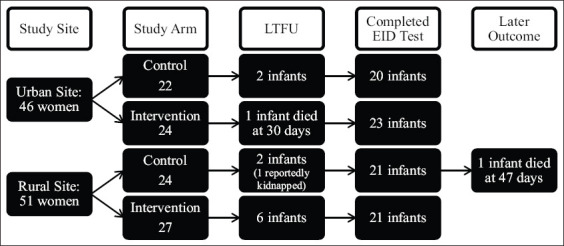
At two sites in Uganda, the Wise Infant Study (WIN) prospectively followed an infant cohort. Infants were born to women enrolled in an RCT testing the effect of real-time reminders delivered via EDM on maternal adherence to antiretroviral therapy. We assessed intrapartum and discharge receipt of NVP prophylaxis using pharmacy and infant HIV DNA testing laboratory data.
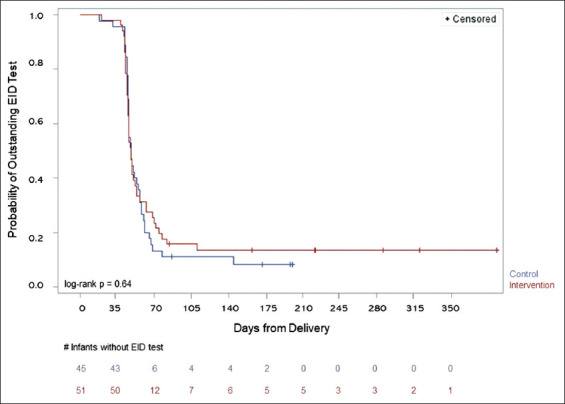
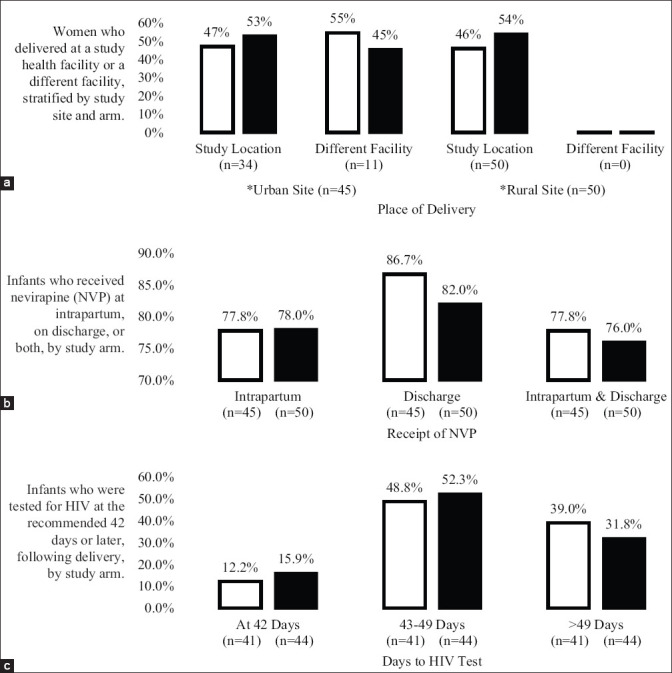
Of 121 women eligible for WIN, 97 (80%) consented and enrolled; 46 had been randomized to control and 51 to intervention. There were no differences in receipt of a six-week NVP supply (control 87%, intervention 82%, p = 0.53). Receipt of any NVP prophylaxis did not vary by delivery location (p = 0.35), and although 12% of infants were delivered at non-study health facilities, they were not less likely to receive NVP at discharge (p = 0.37). Among infants with a completed HIV test, there was no difference in mean time to first test (control 52 days (SD 18), intervention 51 days (SD 15), p = 0.86). Only one infant, in the control group, tested positive for HIV.
We found no significant differences in adherence to infant PMTCT practices between intervention and control infants with relatively high rates of NVP receipt albeit with suboptimal adherence to six-week EID testing. Further work is needed to ensure improved access, uptake, and follow-up of HIV-exposed infants in the Option B+ era.
乌干达已通过预防母婴传播艾滋病毒(PMTCT)项目成功减少了儿童艾滋病毒感染,但对于干预措施中针对婴儿的特定组成部分的依从性了解甚少。我们假设,母亲接受基于WiseMama(WM)电子药物监测(EDM)的依从性干预措施所生的婴儿,其产后六周奈韦拉平(NVP)婴儿预防用药的接受率会提高,并且对六周早期婴儿诊断(EID)艾滋病毒检测的依从性会更好。
在乌干达的两个地点,开展了Wise婴儿研究(WIN),对一个婴儿队列进行前瞻性跟踪。这些婴儿的母亲参加了一项随机对照试验,该试验测试通过EDM提供实时提醒对母亲抗逆转录病毒治疗依从性的影响。我们利用药房和婴儿艾滋病毒DNA检测实验室数据评估了分娩时及出院时NVP预防用药的接受情况。
在121名符合WIN条件的女性中,97名(80%)同意并参与;46名被随机分配到对照组,51名被分配到干预组。六周NVP供应的接受情况没有差异(对照组87%,干预组82%,p = 0.53)。任何NVP预防用药的接受情况在分娩地点方面没有差异(p = 0.35),尽管12%的婴儿在非研究医疗机构出生,但他们出院时接受NVP的可能性并不更低(p = 0.37)。在完成艾滋病毒检测的婴儿中,首次检测的平均时间没有差异(对照组52天(标准差18),干预组51天(标准差15),p = 0.86)。对照组中只有一名婴儿艾滋病毒检测呈阳性。
我们发现,干预组婴儿和对照组婴儿在婴儿PMTCT措施的依从性方面没有显著差异,NVP接受率相对较高,尽管六周EID检测的依从性不理想。在“选项B+”时代,需要进一步努力以确保改善艾滋病毒暴露婴儿的可及性、接受率和随访情况。