Ohio State University, Columbus, Ohio 43210, USA.
J Am Coll Cardiol. 2010 Jun 1;55(22):2480-8. doi: 10.1016/j.jacc.2010.01.047.
The aim of this study was to define the prevalence and significance of myocardial edema in patients with non-ST-segment elevation acute coronary syndrome (NSTE-ACS).
Most patients with NSTE-ACS undergo angiography, yet not all have obstructive coronary artery disease (CAD) requiring revascularization. Identifying patients with myocardium at risk could enhance the effectiveness of an early invasive strategy. Cardiac magnetic resonance (CMR) can demonstrate edematous myocardium subjected to ischemia but has not been used to evaluate NSTE-ACS patients.
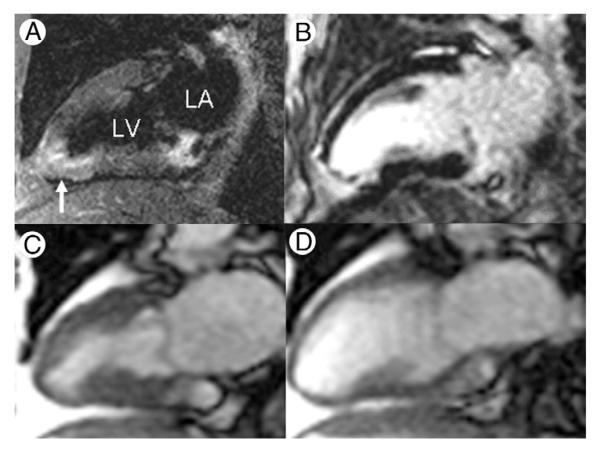
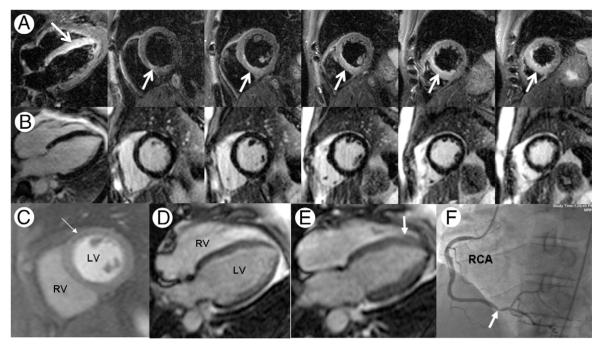
One hundred consecutive patients with NSTE-ACS were prospectively enrolled to undergo 30-min CMR, including T2-weighted edema imaging and late gadolinium enhancement before coronary angiography. Clinical management including revascularization decision-making was performed without CMR results.
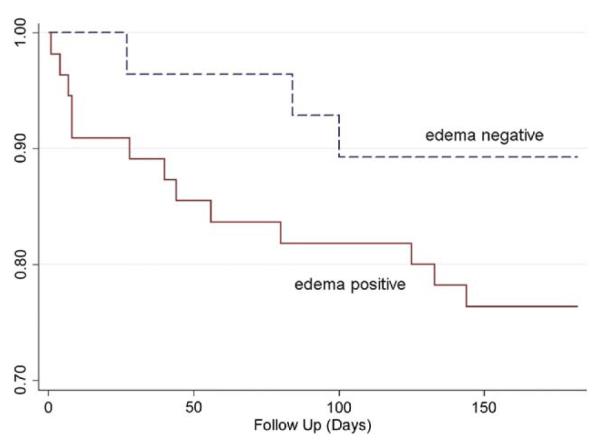
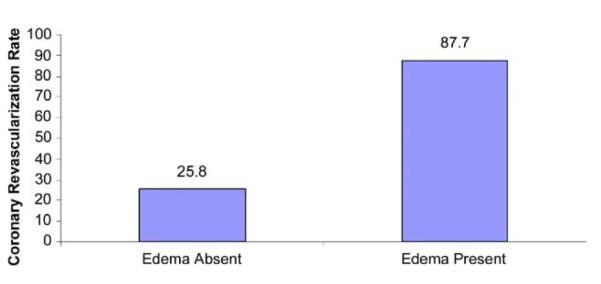
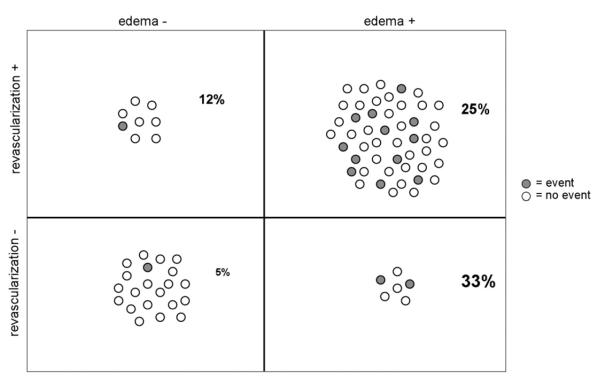
Of 88 adequate CMR studies, 57 (64.8%) showed myocardial edema. Obstructive CAD requiring revascularization was present in 87.7% of edema-positive patients versus 25.8% of edema-negative patients (p < 0.001). By multiple logistic regression analysis after adjusting for late gadolinium enhancement, perfusion, and wall motion scores, TIMI risk score was not predictive of obstructive CAD. Conversely, an increase in T2 score by 1 U increased the odds of subsequent coronary revascularization by 5.70 times (95% confidence interval: 2.38 to 13.62, p < 0.001). Adjusting for peak troponin-I, patients with edema showed a higher hazard of a cardiovascular event or death within 6 months after NSTE-ACS compared with those without edema (hazard ratio: 4.47, 95% confidence interval: 1.00 to 20.03; p = 0.050).
In NSTE-ACS patients, rapid CMR identifies reversibly injured myocardium due to obstructive CAD and predicts worse outcomes. Identifying myocardium at risk may help direct appropriate patients toward early invasive management.
本研究旨在定义非 ST 段抬高型急性冠状动脉综合征(NSTE-ACS)患者心肌水肿的患病率和意义。
大多数 NSTE-ACS 患者接受血管造影,但并非所有患者都存在需要血运重建的阻塞性冠状动脉疾病(CAD)。识别有心肌风险的患者可以提高早期侵入性策略的效果。心脏磁共振(CMR)可显示缺血导致的水肿性心肌,但尚未用于评估 NSTE-ACS 患者。
前瞻性纳入 100 例 NSTE-ACS 患者,行 30 分钟 CMR,包括 T2 加权水肿成像和血管造影前晚期钆增强。临床管理包括血运重建决策,而不考虑 CMR 结果。
在 88 例充分 CMR 研究中,57 例(64.8%)显示心肌水肿。在水肿阳性患者中,需要血运重建的阻塞性 CAD 占 87.7%,而在水肿阴性患者中占 25.8%(p<0.001)。经调整晚期钆增强、灌注和壁运动评分后的多变量逻辑回归分析,TIMI 风险评分不能预测阻塞性 CAD。相反,T2 评分增加 1 U,随后进行冠状动脉血运重建的几率增加 5.70 倍(95%置信区间:2.38 至 13.62,p<0.001)。调整峰值肌钙蛋白 I 后,与无水肿患者相比,有水肿的患者在 NSTE-ACS 后 6 个月内发生心血管事件或死亡的风险更高(危险比:4.47,95%置信区间:1.00 至 20.03;p=0.050)。
在 NSTE-ACS 患者中,快速 CMR 可识别因阻塞性 CAD 导致的可逆性损伤心肌,并预测更差的结局。识别有风险的心肌可能有助于指导适当的患者进行早期侵入性治疗。