Kwai Chung Hospital, Hospital Authority, Hong Kong S.A.R., China.
J Neurogastroenterol Motil. 2010 Jan;16(1):52-60. doi: 10.5056/jnm.2010.16.1.52. Epub 2010 Jan 31.
Psychiatric comorbidity is common in patients with functional dyspepsia (FD) but a good screening tool for psychiatric disorders in gastrointestinal clinical practice is lacking.
Consecutive patients fulfilling Rome III criteria for FD without medical co-morbidities and gastroesophageal reflux disease were recruited in a gastroenterology clinic. The followings were conducted at 4 weeks after index oesophagogastroduodenoscopy: self-administrated questionnaires on socio-demographics, dyspeptic symptom severity (4-point Likert scale), GHQ-12, and 36-item short-form health survey (SF-36). Psychiatric disorders were diagnosed with Structured Clinical Interview for DSM-IV Axis I Disorders (SCID) by a trained psychiatrist, which served as reference standard.
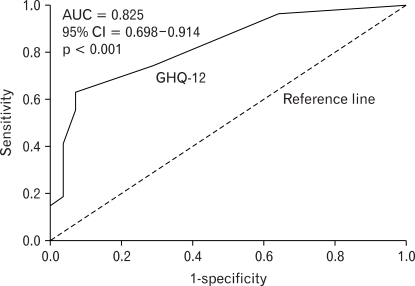
55 patients underwent psychiatrist-conducted interview and questionnaire assessment. 27 (49.1%) had current psychiatric disorders as determined by SCID (anxiety disorders: 38.2%, depressive disorders: 16.4%). Receiver operating characteristic curve analysis of GHQ-12 revealed an area under curve of 0.825 (95%CI: 0.698-0.914). Cut-off of GHQ-12 at >/=3 gave a sensitivity of 63.0% (95%CI = 42.4-80.6%) and specificity of 92.9% (95%CI = 76.5%-98.9%). Subjects with co-existing psychiatric disorders scored significantly lower in multiple domains of SF-36 (mental component summary, general health, vitality and mental health). By multivariate linear regression analysis, current psychiatric morbidities (Beta = -0.396, p = 0.002) and family history of psychiatric illness (Beta = -0.299, p = 0.015) were independent risk factors for poorer mental component summary in SF-36, while dyspepsia severity was the only independent risk factor for poorer physical component summary (Beta = -0.332, p = 0.027).
Concomitant psychiatric disorders adversely affect HRQoL in FD patients. The use of GHQ-12 as a reliable screening tool for psychiatric disorders allows early intervention and may improve clinical outcomes of these patients.
功能性消化不良(FD)患者常伴有精神共病,但在胃肠临床实践中缺乏有效的精神障碍筛查工具。
1)评估 12 项一般健康问卷(GHQ-12)作为 FD 患者精神障碍筛查工具的性能和最佳截断值;2)比较伴有和不伴有精神共病的 FD 患者的健康相关生活质量(HRQoL)。
在消化内科门诊连续招募符合 Rome III 标准且无合并症和胃食管反流病的 FD 患者。在索引食管胃十二指肠镜检查后 4 周进行以下检查:自我管理的社会人口统计学问卷、消化不良症状严重程度(4 分 Likert 量表)、GHQ-12 和 36 项简明健康调查(SF-36)。精神障碍采用经过培训的精神科医生进行的 DSM-IV 轴 I 障碍结构化临床访谈(SCID)进行诊断,作为参考标准。
55 例患者接受了精神科医生进行的访谈和问卷调查评估。27 例(49.1%)根据 SCID 确定存在当前精神障碍(焦虑障碍:38.2%,抑郁障碍:16.4%)。GHQ-12 的受试者工作特征曲线分析显示曲线下面积为 0.825(95%CI:0.698-0.914)。GHQ-12>3 分的截断值具有 63.0%的敏感性(95%CI=42.4-80.6%)和 92.9%的特异性(95%CI=76.5%-98.9%)。同时患有精神障碍的患者在 SF-36 的多个领域评分明显较低(心理成分综合评分、一般健康、活力和心理健康)。通过多元线性回归分析,当前精神疾病(β=-0.396,p=0.002)和精神疾病家族史(β=-0.299,p=0.015)是 SF-36 心理成分综合评分较差的独立危险因素,而消化不良严重程度是物理成分综合评分较差的唯一独立危险因素(β=-0.332,p=0.027)。
并存的精神障碍会对 FD 患者的 HRQoL 产生不利影响。使用 GHQ-12 作为精神障碍的可靠筛查工具可以进行早期干预,并可能改善这些患者的临床结局。