Department of Intensive Care Medicine, Bern University Hospital and University of Bern Inselspital, Freiburgstrasse 10, 3010 Bern, Switzerland.
Crit Care. 2010;14(3):R111. doi: 10.1186/cc9060. Epub 2010 Jun 11.
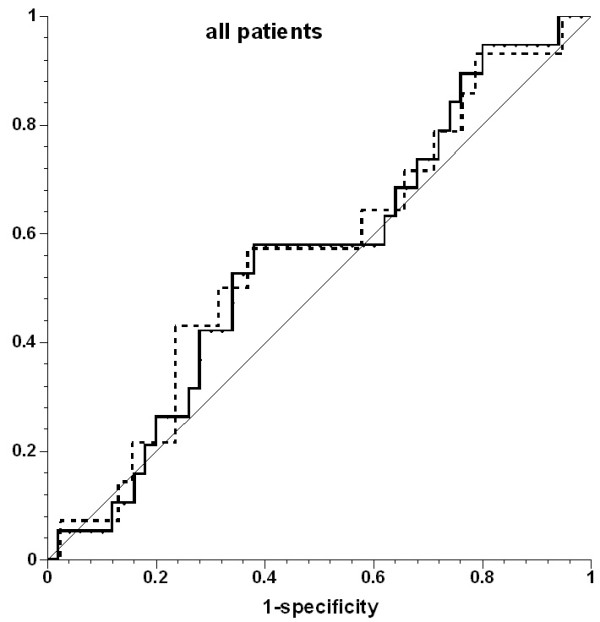
Pulse-pressure variation (PPV) due to increased right ventricular afterload and dysfunction may misleadingly suggest volume responsiveness. We aimed to assess prediction of volume responsiveness with PPV in patients with increased pulmonary artery pressure.
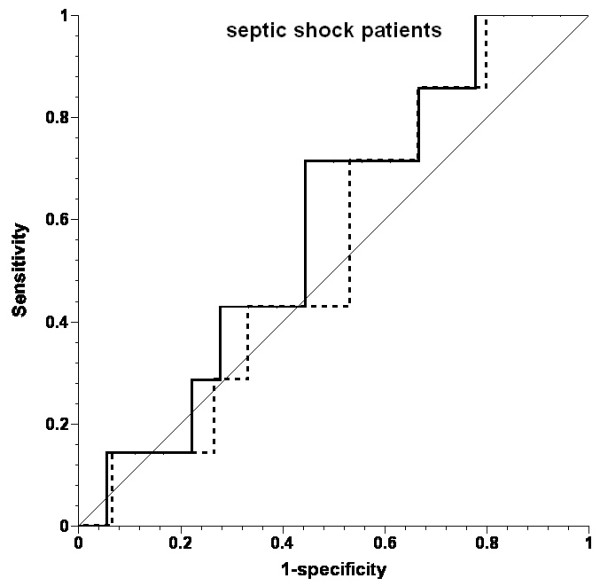
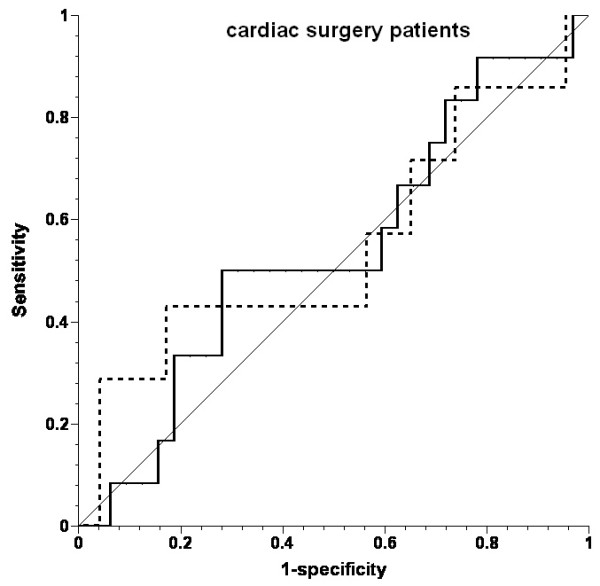
Fifteen cardiac surgery patients with a history of increased pulmonary artery pressure (mean pressure, 27 +/- 5 mm Hg (mean +/- SD) before fluid challenges) and seven septic shock patients (mean pulmonary artery pressure, 33 +/- 10 mm Hg) were challenged with 200 ml hydroxyethyl starch boli ordered on clinical indication. PPV, right ventricular ejection fraction (EF) and end-diastolic volume (EDV), stroke volume (SV), and intravascular pressures were measured before and after volume challenges.
Of 69 fluid challenges, 19 (28%) increased SV > 10%. PPV did not predict volume responsiveness (area under the receiver operating characteristic curve, 0.555; P = 0.485). PPV was >or=13% before 46 (67%) fluid challenges, and SV increased in 13 (28%). Right ventricular EF decreased in none of the fluid challenges, resulting in increased SV, and in 44% of those in which SV did not increase (P = 0.0003). EDV increased in 28% of fluid challenges, resulting in increased SV, and in 44% of those in which SV did not increase (P = 0.272).
Both early after cardiac surgery and in septic shock, patients with increased pulmonary artery pressure respond poorly to fluid administration. Under these conditions, PPV cannot be used to predict fluid responsiveness. The frequent reduction in right ventricular EF when SV did not increase suggests that right ventricular dysfunction contributed to the poor response to fluids.
由于右心室后负荷增加和功能障碍导致的脉压变化(PPV)可能会误导性地提示容量反应性。我们旨在评估在肺动脉压升高的患者中,使用 PPV 预测容量反应性。
15 例有肺动脉压升高病史的心脏手术患者(液体挑战前平均压为 27 ± 5 mmHg(平均值 ± 标准差))和 7 例脓毒性休克患者(平均肺动脉压为 33 ± 10 mmHg)根据临床指征接受 200 ml 羟乙基淀粉冲击。在容量挑战前后测量 PPV、右心室射血分数(EF)和舒张末期容积(EDV)、每搏量(SV)和血管内压力。
69 次液体挑战中,19 次(28%)SV 增加>10%。PPV 不能预测容量反应性(ROC 曲线下面积,0.555;P = 0.485)。在 46 次(67%)液体挑战前,PPV>or=13%,SV 增加 13 次(28%)。在没有液体挑战的情况下,右心室 EF 没有下降,导致 SV 增加,而在 SV 没有增加的情况下,有 44%(P = 0.0003)。在 28%的液体挑战中,EDV 增加,导致 SV 增加,而在 SV 没有增加的情况下,有 44%(P = 0.272)。
在心脏手术后早期和脓毒性休克中,肺动脉压升高的患者对液体治疗反应不佳。在这些情况下,PPV 不能用于预测液体反应性。当 SV 没有增加时,右心室 EF 经常下降,这表明右心室功能障碍导致对液体的反应不佳。