School of Health Sciences, University of Southampton, Southampton, UK.
NIHR Musculoskeletal Biomedical Research Unit, University of Oxford, Oxford, UK.
J Foot Ankle Res. 2010 Jun 17;3:10. doi: 10.1186/1757-1146-3-10.
Inhibition of tumour necrosis factor (TNF) is an effective way of reducing synovitis and preventing joint damage in rheumatoid arthritis (RA), yet very little is known about its specific effect on foot pain and disability. The aim of this study was to evaluate whether anti-TNF therapy alters the presence of forefoot pathology and/or reduces foot pain and disability.
Consecutive RA patients starting anti-TNF therapy (infliximab, etanercept, adalimumab) were assessed for presence of synovial hypertrophy and synovitis in the 2nd and 5th metatarso-phalangeal (MTP) joints and plantar forefoot bursal hypertrophy before and 12 weeks after therapy. Tender MTP joints and swollen bursae were established clinically by an experienced podiatrist and ultrasound (US) images were acquired and interpreted by a radiologist. Assessment of patient reported disease impact on the foot was performed using the Manchester Foot Pain and Disability Index (MFPDI).
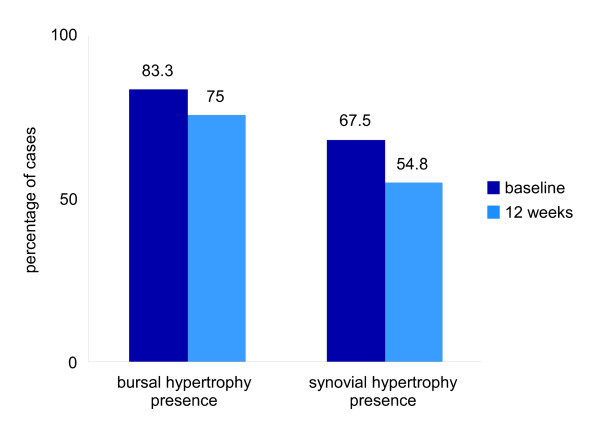
31 patients (24 female, 7 male) with RA (12 seronegative, 19 seropositive) completed the study: mean age 59.6 (SD 10.1) years, disease duration 11.1 (SD 10.5) years, and previous number of Disease Modifying Anti Rheumatic Drugs 3.0 (1.6). Significant differences after therapy were found for Erythrocyte Sedimentation Rate (t = 4.014, p < 0.001), C-reactive protein (t = 3.889, p = 0.001), 28 joint Disease Activity Score (t = 3.712, p = 0.0001), Visual Analog Scale (t = 2.735, p = 0.011) and Manchester Foot Pain and Disability Index (t = 3.712, p = 0.001).Presence of MTP joint synovial hypertrophy on US was noted in 67.5% of joints at baseline and 54.8% of joints at twelve weeks. Presence of plantar forefoot bursal hypertrophy on US was noted in 83.3% of feet at baseline and 75% at twelve weeks. Although there was a trend for reduction in observed presence of person specific forefoot pathology, when the frequencies were analysed (McNemar) this was not significant.
Significant improvements were seen in patient reported foot pain and disability 12 weeks after commencing TNF inhibition in RA, but this may not be enough time to detect changes in forefoot pathology.
抑制肿瘤坏死因子(TNF)是减轻类风湿关节炎(RA)滑膜炎和预防关节损伤的有效方法,但对于其对足部疼痛和残疾的具体影响知之甚少。本研究旨在评估抗 TNF 治疗是否改变了前足病理的存在,并/或减轻了足部疼痛和残疾。
连续接受抗 TNF 治疗(英夫利昔单抗、依那西普、阿达木单抗)的 RA 患者,在治疗前和治疗后 12 周,评估第 2 和第 5 跖跗(MTP)关节和足底前足滑囊的滑膜肥厚和滑膜炎。经验丰富的足病医生通过临床检查确定压痛 MTP 关节和肿胀滑囊,放射科医生采集和解释超声(US)图像。采用曼彻斯特足部疼痛和残疾指数(MFPDI)评估患者报告的足部疾病对其的影响。
31 名(24 名女性,7 名男性)RA 患者(12 名血清阴性,19 名血清阳性)完成了这项研究:平均年龄 59.6(SD 10.1)岁,病程 11.1(SD 10.5)年,之前使用的疾病修饰抗风湿药物为 3.0(1.6)。治疗后发现红细胞沉降率(t = 4.014,p < 0.001)、C 反应蛋白(t = 3.889,p = 0.001)、28 关节疾病活动评分(t = 3.712,p = 0.0001)、视觉模拟评分(t = 2.735,p = 0.011)和曼彻斯特足部疼痛和残疾指数(t = 3.712,p = 0.001)均有显著差异。治疗前,67.5%的关节在 US 上可见 MTP 关节滑膜肥厚,12 周时为 54.8%。治疗前,83.3%的足部在 US 上可见足底前足滑囊肥厚,12 周时为 75%。尽管观察到特定患者前足病理存在的减少趋势,但在对频率进行分析(McNemar)时,这并不显著。
RA 患者开始接受 TNF 抑制治疗 12 周后,患者报告的足部疼痛和残疾明显改善,但这可能不足以检测到前足病理的变化。