Division of Cardiology, Careggi Hospital, Florence, Italy.
J Thromb Thrombolysis. 2010 Nov;30(4):446-51. doi: 10.1007/s11239-010-0481-5.
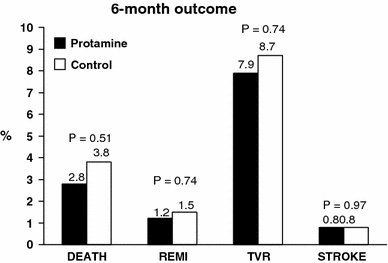
Infarct artery stenting with adjunctive abciximab therapy is widely used treatment for patients with acute myocardial infarction (AMI). However, bleeding complications have been associated with a worse clinical outcome. Randomized trials in elective patients have shown that postprocedural protamine administration is safe and associated with a significant reduction in bleeding complications. The aim of the current study was to evaluate in STEMI patients undergoing primary percutaneous coronary intervention (PCI) with abciximab and stenting whether immediate reversal of anticoagulation by protamine is safe and associated with a reduction in the occurrence of bleeding complications. From January 2004 to June 2005, 254 patients with STEMI had immediate reversal of anticoagulation by protamine administration after infarct artery stenting and received abciximab therapy without heparin infusion (Group 1). These patients were compared with a control group of 265 patients (June 2002-December 2003) treated with the standard heparin therapy: bolus in order to achieve an activated coagulation time of 250-300 s during PCI plus 12-h infusion (7 UI/kg/h; Group 2). We excluded patients undergoing IABP implantation. The two groups were similar in all baseline characteristics. There were no differences in in-hospital mortality, reinfarction, urgent target vessel revascularization, stroke or acute or subacute stent thrombosis, while Group 1 patients showed a lower incidence of major bleeding complications (ACUITY scale: 1.1 vs. 4.0%, P = 0.035) and a shorter length of hospital stay (3.5 ± 1.7 vs. 4.0 ± 1.6 days, P = 0.002) as compared with heparin treated patients. Among patients undergoing primary stenting with abciximab administration, immediate post-PCI reversal anticoagulation by protamine without associated heparin infusion is safe and associated with a significant reduction in major bleeding complications.
急性心肌梗死(AMI)患者常采用经皮冠状动脉介入治疗(PCI)联合替罗非班进行梗死相关动脉血运重建。然而,出血并发症与临床预后不良相关。在择期患者的随机临床试验中,研究发现术后应用鱼精蛋白中和肝素是安全的,且能显著减少出血并发症。本研究旨在探讨替罗非班联合 PCI 治疗 ST 段抬高型心肌梗死(STEMI)患者中,即刻应用鱼精蛋白逆转抗凝治疗是否安全,以及是否可以减少出血并发症。从 2004 年 1 月至 2005 年 6 月,254 例 STEMI 患者接受 PCI 联合支架置入治疗后即刻应用鱼精蛋白中和抗凝,并在未接受肝素输注的情况下应用替罗非班(替罗非班组)。与标准肝素治疗(肝素组)的 265 例患者进行比较,肝素组术中予肝素负荷剂量(使活化凝血时间达 250-300s),术后持续 12 小时输注(7UI/kg/h)。排除接受主动脉内球囊反搏术(IABP)治疗的患者。两组患者基线资料相似。替罗非班组住院期间死亡率、再梗死、紧急靶血管血运重建、卒中和急性或亚急性支架血栓形成发生率与肝素组无差异,替罗非班组主要出血并发症发生率(ACUITY 评分)明显低于肝素组(1.1%比 4.0%,P=0.035),住院时间明显短于肝素组(3.5±1.7 比 4.0±1.6 天,P=0.002)。在接受替罗非班联合 PCI 治疗的患者中,即刻应用鱼精蛋白中和替罗非班,不联合肝素输注是安全的,且可显著减少主要出血并发症。