VA National Quality Scholars Program, Department of Veterans Affairs Medical Center, Birmingham, AL, USA.
Implement Sci. 2010 Jul 19;5:55. doi: 10.1186/1748-5908-5-55.
Multiple uncontrolled medical conditions may act as competing demands for clinical decision making. We hypothesized that multiple uncontrolled cardiovascular risk factors would decrease blood pressure (BP) medication intensification among uncontrolled hypertensive patients.
We observed 946 encounters at two VA primary care clinics from May through August 2006. After each encounter, clinicians recorded BP medication intensification (BP medication was added or titrated). Demographic, clinical, and laboratory information were collected from the medical record. We examined BP medication intensification by presence and control of diabetes and/or hyperlipidemia. 'Uncontrolled' was defined as hemoglobin A1c >/= for diabetes, BP >/= 140/90 mmHg (>/= 130/80 mmHg if diabetes present) for hypertension, and low density lipoprotein cholesterol (LDL-c) >/= 130 mg/dl (>/= 100 mg/dl if diabetes present) for hyperlipidemia. Hierarchical regression models accounted for patient clustering and adjusted medication intensification for age, systolic BP, and number of medications.
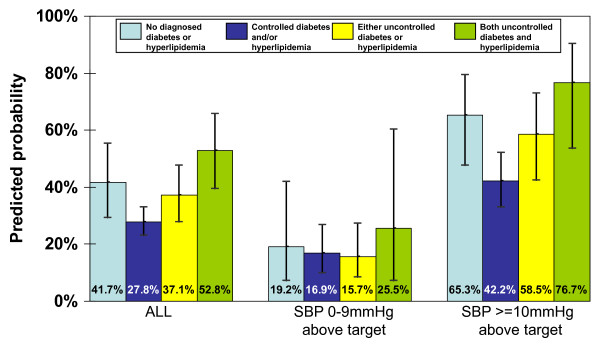
Among 387 patients with uncontrolled hypertension, 51.4% had diabetes (25.3% were uncontrolled) and 73.4% had hyperlipidemia (22.7% were uncontrolled). The BP medication intensification rate was 34.9% overall, but higher in individuals with uncontrolled diabetes and uncontrolled hyperlipidemia: 52.8% overall and 70.6% if systolic BP >/= 10 mmHg above goal. Intensification rates were lowest if diabetes or hyperlipidemia were controlled, lower than if diabetes or hyperlipidemia were not present. Multivariable adjustment yielded similar results.
The presence of uncontrolled diabetes and hyperlipidemia was associated with more guideline-concordant hypertension care, particularly if BP was far from goal. Efforts to understand and improve BP medication intensification in patients with controlled diabetes and/or hyperlipidemia are warranted.
多种不受控制的医疗状况可能成为临床决策的竞争需求。我们假设,存在多种不受控制的心血管风险因素会降低高血压患者血压(BP)药物的强化治疗率。
我们观察了 2006 年 5 月至 8 月期间在两家退伍军人事务部(VA)初级保健诊所的 946 次就诊。每次就诊后,临床医生记录 BP 药物的强化治疗情况(添加或调整 BP 药物)。从病历中收集人口统计学、临床和实验室信息。我们通过存在和控制糖尿病和/或高脂血症来检查 BP 药物的强化治疗情况。“不受控制”定义为血红蛋白 A1c >/= 糖尿病,高血压为 BP >/= 140/90mmHg(糖尿病存在时>/= 130/80mmHg),高脂血症为低密度脂蛋白胆固醇(LDL-c)>/= 130mg/dl(糖尿病存在时>/= 100mg/dl)。分层回归模型考虑了患者聚类,并根据年龄、收缩压和药物种类调整了药物强化治疗。
在 387 例高血压未控制的患者中,51.4%有糖尿病(25.3%未控制),73.4%有高脂血症(22.7%未控制)。总体而言,BP 药物强化治疗率为 34.9%,但在未控制的糖尿病和未控制的高脂血症患者中更高:总体为 52.8%,如果收缩压比目标高>/= 10mmHg,则为 70.6%。如果糖尿病或高脂血症得到控制,强化治疗率最低,低于如果糖尿病或高脂血症不存在的情况。多变量调整后得出了相似的结果。
存在未控制的糖尿病和高脂血症与更符合指南的高血压治疗相关,特别是如果血压远远低于目标。有必要努力了解和改善控制了糖尿病和/或高脂血症患者的 BP 药物强化治疗情况。