Breast Research Group, University of Edinburgh, Western General Hospital, Crewe Road South, Edinburgh EH4 2XU, UK.
Breast Cancer Res. 2010;12(4):R52. doi: 10.1186/bcr2611. Epub 2010 Jul 20.
Clinical resistance is a major factor limiting benefits to endocrine therapy. Causes of resistance may be diverse and the mechanism of resistance in individual breast cancers is usually unknown. The present study illustrates how changes in the expression of proliferation and oestrogen-regulated genes occurring during neoadjuvant treatment with the aromatase inhibitor, letrozole, may define distinctive tumour subgroups and suggest different mechanisms of resistance in clinically endocrine resistant breast cancers.
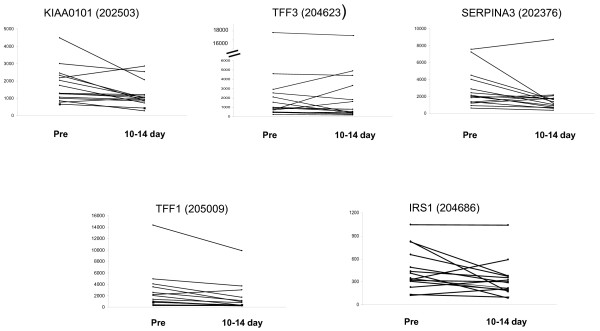
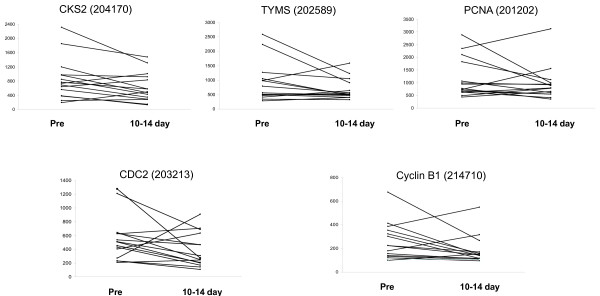
Postmenopausal women with large primary oestrogen-receptor (ER)-rich breast cancers were treated neoadjuvantly with letrozole (2.5 mg daily) for three months. Clinical response was determined by ultrasound changes in tumour volume. Tumour ribonucleic acid (RNA) from biopsies taken before, after 14 days and after three months of treatment was hybridized on Affymetrix U133A chips. Changes in expression of KIAA0101, TFF3, SERPINA3, IRS-1 and TFF1 were taken as markers of oestrogen regulation and those in CDC2, CKS-2, Cyclin B1, Thymidine Synthetase and PCNA as markers of proliferation.
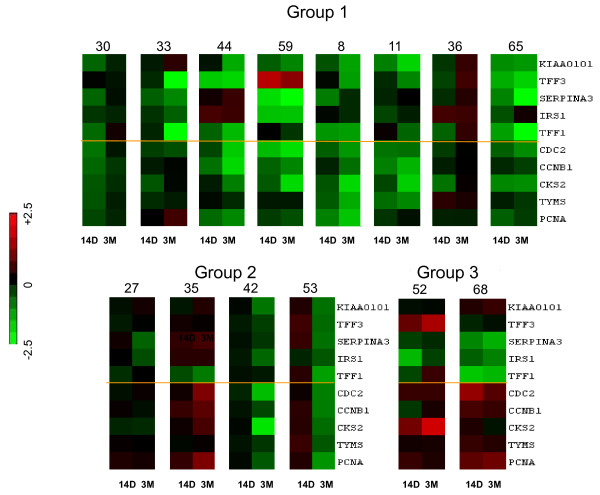
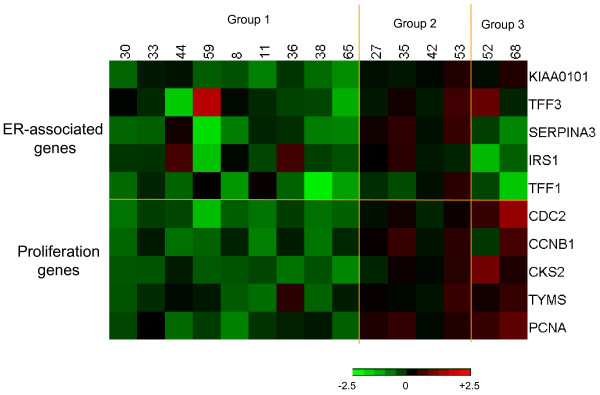
Fifteen tumours with < 50% volume reduction over three months of treatment were classified as being clinically non-responsive. Gene expression changes after 14 days of treatment with letrozole revealed different patterns of change in oestrogen regulated and proliferation genes in individual resistant tumours. Tumours could be separated into three different subgroups as follows: i) nine cases in which both proliferation and oestrogen signalling signatures were generally reduced on treatment (ii) four cases in which both signatures were generally unaffected or increased with treatment and (iii) two cases in which expression of the majority of oestrogen-regulated genes decreased whereas proliferation genes remained unchanged or increased. In 14 out of 15 tumours, RNA profiles were also available after three months of treatment. Patterns of change observed after 14 days were maintained or accentuated at three months in nine tumours but changes in patterns were apparent in the remaining five cancers.
Different dynamic patterns of expression of oestrogen-regulated and proliferation genes were observed in tumours clinically resistant to neoadjuvant letrozole, thus illustrating heterogeneity of resistance and discriminating molecular sub-classes of resistant tumours. Molecular phenotyping might help to direct circumventing therapy suggesting the targeting of specific pathways in different tumour subtypes.
临床耐药是限制内分泌治疗获益的主要因素。耐药的原因可能多种多样,而且个体乳腺癌的耐药机制通常是未知的。本研究说明了在新辅助治疗中使用芳香酶抑制剂来曲唑时,增殖和雌激素调节基因表达的变化如何定义不同的肿瘤亚群,并提示临床内分泌耐药乳腺癌中不同的耐药机制。
绝经后患有大的原发性雌激素受体(ER)丰富的乳腺癌患者接受来曲唑(2.5mg 每日)新辅助治疗 3 个月。通过肿瘤体积超声变化确定临床反应。在治疗前、治疗 14 天后和 3 个月后取活检的肿瘤核糖核酸(RNA)在 Affymetrix U133A 芯片上杂交。将 KIAA0101、TFF3、SERPINA3、IRS-1 和 TFF1 的表达变化作为雌激素调节的标志物,将 CDC2、CKS-2、Cyclin B1、胸苷合成酶和 PCNA 的表达变化作为增殖的标志物。
15 例在 3 个月的治疗过程中肿瘤体积减少<50%的患者被归类为临床无反应。来曲唑治疗 14 天后基因表达的变化显示,个别耐药肿瘤中雌激素调节和增殖基因的变化模式不同。肿瘤可以分为以下三个不同的亚组:i)9 例在治疗过程中增殖和雌激素信号特征均普遍降低;ii)4 例在治疗过程中这两个特征均未受影响或增加;iii)2 例多数雌激素调节基因表达减少而增殖基因保持不变或增加。在 15 例肿瘤中,14 例在治疗 3 个月后也有 RNA 谱。在 9 例肿瘤中,14 天观察到的变化模式在 3 个月时保持或加重,但在其余 5 例肿瘤中变化模式发生了改变。
在新辅助来曲唑治疗临床耐药的肿瘤中观察到雌激素调节和增殖基因表达的不同动态模式,这表明了耐药的异质性,并区分了耐药肿瘤的分子亚群。分子表型可能有助于指导绕过治疗,提示针对不同肿瘤亚型的特定途径。