Combimatrix Molecular Diagnostics, 310 Goddard, Irvine, California 92618, USA.
BMC Cancer. 2010 Jul 28;10:396. doi: 10.1186/1471-2407-10-396.
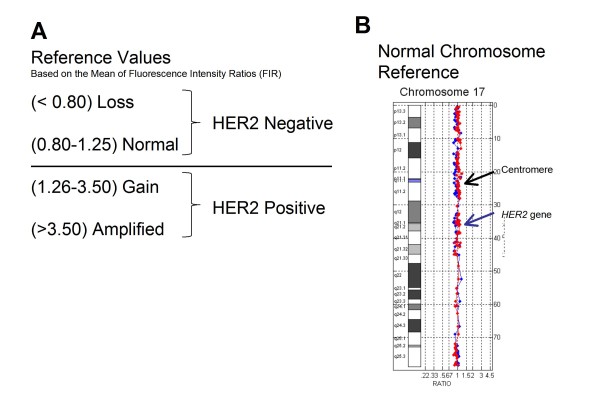
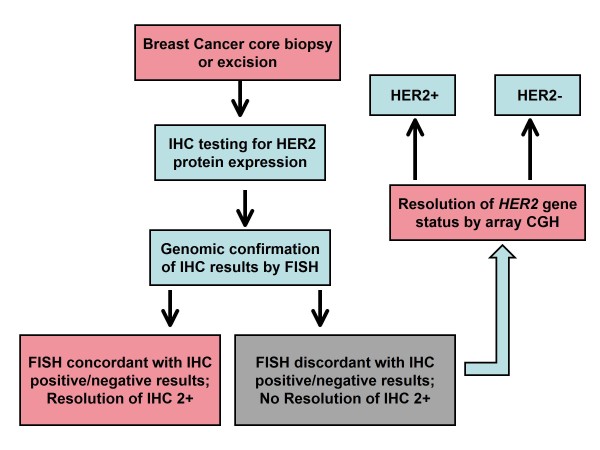
HER2 gene copy status, and concomitant administration of trastuzumab (Herceptin), remains one of the best examples of targeted cancer therapy based on understanding the genomic etiology of disease. However, newly diagnosed breast cancer cases with equivocal HER2 results present a challenge for the oncologist who must make treatment decisions despite the patient's unresolved HER2 status. In some cases both immunohistochemistry (IHC) and fluorescence in situ hybridization (FISH) are reported as equivocal, whereas in other cases IHC results and FISH are discordant for positive versus negative results. The recent validation of array-based, molecular karyotyping for clinical oncology testing provides an alternative method for determination of HER2 gene copy number status in cases remaining unresolved by traditional methods.
In the current study, DNA extracted from 20 formalin fixed paraffin embedded (FFPE) tissue samples from newly diagnosed cases of invasive ductal carcinoma referred to our laboratory with unresolved HER2 status, were analyzed using a clinically validated genomic array containing 127 probes covering the HER2 amplicon, the pericentromeric regions, and both chromosome 17 arms.
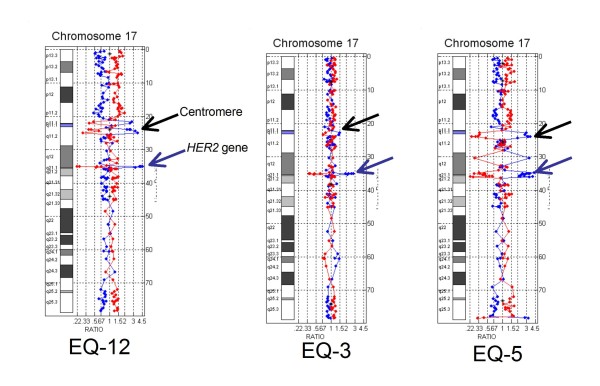
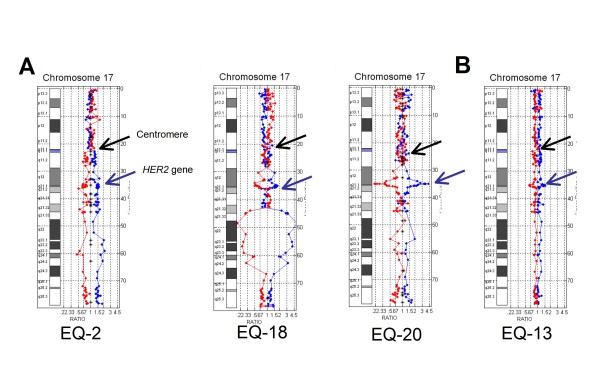
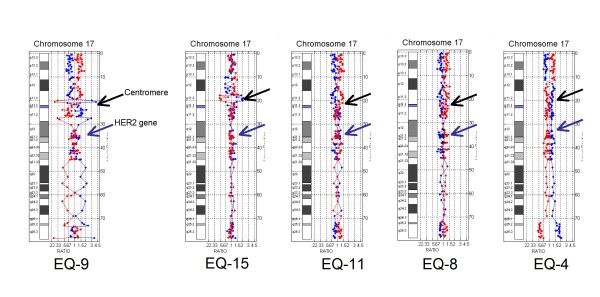
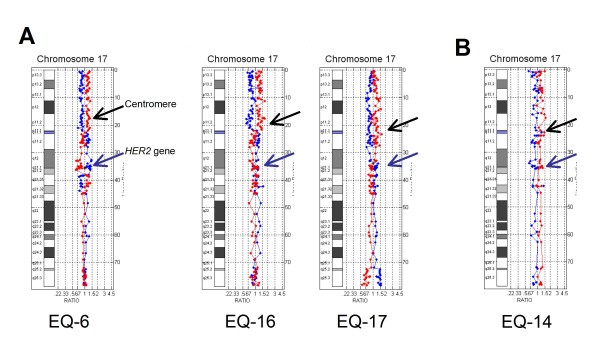
Array-based comparative genomic hybridization (array CGH) analysis of chromosome 17 resolved HER2 gene status in [20/20] (100%) of cases and revealed additional chromosome 17 copy number changes in [18/20] (90%) of cases. Array CGH analysis also revealed two false positives and one false negative by FISH due to "ratio skewing" caused by chromosomal gains and losses in the centromeric region. All cases with complex rearrangements of chromosome 17 showed genome-wide chromosomal instability.
These results illustrate the analytical power of array-based genomic analysis as a clinical laboratory technique for resolution of HER2 status in breast cancer cases with equivocal results. The frequency of complex chromosome 17 abnormalities in these cases suggests that the two probe FISH interphase analysis is inadequate and results interpreted using the HER2/CEP17 ratio should be reported "with caution" when the presence of centromeric amplification or monosomy is suspected by FISH signal gains or losses. The presence of these pericentromeric copy number changes may result in artificial skewing of the HER2/CEP17 ratio towards false negative or false positive results in breast cancer with chromosome 17 complexity. Full genomic analysis should be considered in all cases with complex chromosome 17 aneusomy as these cases are likely to have genome-wide instability, amplifications, and a poor prognosis.
基于对疾病基因组病因的理解,HER2 基因拷贝状态以及曲妥珠单抗(赫赛汀)的同时使用仍然是基于靶向癌症治疗的最佳范例之一。然而,HER2 结果不确定的新诊断乳腺癌病例给肿瘤学家带来了挑战,尽管患者的 HER2 状态尚未解决,他们仍必须做出治疗决策。在某些情况下,免疫组织化学(IHC)和荧光原位杂交(FISH)均报告为不确定,而在其他情况下,IHC 结果和 FISH 对于阳性与阴性结果不一致。最近,基于阵列的分子细胞遗传学检测在临床肿瘤学中的验证为通过传统方法仍未解决的病例确定 HER2 基因拷贝数状态提供了另一种方法。
在目前的研究中,从我们实验室送检的 20 例新诊断为浸润性导管癌的福尔马林固定石蜡包埋(FFPE)组织样本中提取 DNA,这些样本的 HER2 状态不确定,使用经过临床验证的基因组芯片进行分析,该芯片包含 127 个探针,涵盖 HER2 扩增子、着丝粒区域和两条 17 号染色体臂。
基于阵列的比较基因组杂交(array CGH)分析解决了 [20/20](100%)HER2 基因状态,并在 [18/20](90%)病例中揭示了额外的 17 号染色体拷贝数变化。array CGH 分析还揭示了由于“比值倾斜”导致的两个假阳性和一个假阴性,这是由于在着丝粒区域的染色体获得和丢失。所有染色体 17 复杂重排的病例均表现出全基因组染色体不稳定性。
这些结果说明了基于阵列的基因组分析作为一种临床实验室技术的分析能力,可用于解决 HER2 状态不确定的乳腺癌病例。这些病例中复杂的染色体 17 异常的频率表明,当 FISH 信号增益或丢失提示着丝粒扩增或单体性时,使用 HER2/CEP17 比值进行解释的两探针 FISH 间期分析是不充分的,并且应该“谨慎”报告结果。这些着丝粒周围拷贝数变化的存在可能导致乳腺癌中 HER2/CEP17 比值出现人为倾斜,导致假阴性或假阳性结果。在所有染色体 17 非整倍体复杂的病例中都应考虑全基因组分析,因为这些病例可能具有全基因组不稳定性、扩增和不良预后。