Sarin Hemant
National Institute of Biomedical Imaging and Bioengineering, National Institutes of Health, Bethesda, Maryland 20892, USA.
J Angiogenes Res. 2010 Aug 11;2:14. doi: 10.1186/2040-2384-2-14.
Much of our current understanding of microvascular permeability is based on the findings of classic experimental studies of blood capillary permeability to various-sized lipid-insoluble endogenous and non-endogenous macromolecules. According to the classic small pore theory of microvascular permeability, which was formulated on the basis of the findings of studies on the transcapillary flow rates of various-sized systemically or regionally perfused endogenous macromolecules, transcapillary exchange across the capillary wall takes place through a single population of small pores that are approximately 6 nm in diameter; whereas, according to the dual pore theory of microvascular permeability, which was formulated on the basis of the findings of studies on the accumulation of various-sized systemically or regionally perfused non-endogenous macromolecules in the locoregional tissue lymphatic drainages, transcapillary exchange across the capillary wall also takes place through a separate population of large pores, or capillary leaks, that are between 24 and 60 nm in diameter. The classification of blood capillary types on the basis of differences in the physiologic upper limits of pore size to transvascular flow highlights the differences in the transcapillary exchange routes for the transvascular transport of endogenous and non-endogenous macromolecules across the capillary walls of different blood capillary types.
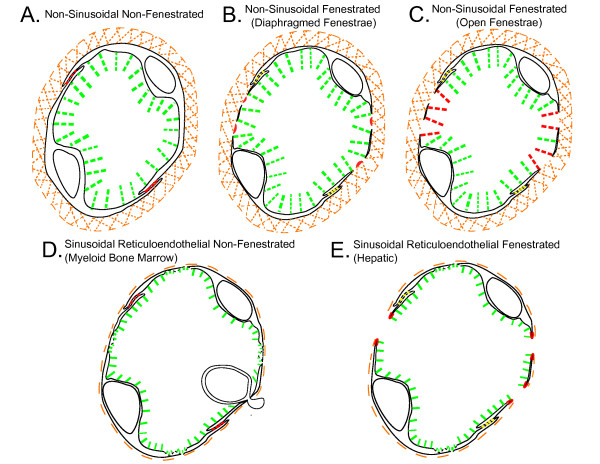
The findings and published data of studies on capillary wall ultrastructure and capillary microvascular permeability to lipid-insoluble endogenous and non-endogenous molecules from the 1950s to date were reviewed. In this study, the blood capillary types in different tissues and organs were classified on the basis of the physiologic upper limits of pore size to the transvascular flow of lipid-insoluble molecules. Blood capillaries were classified as non-sinusoidal or sinusoidal on the basis of capillary wall basement membrane layer continuity or lack thereof. Non-sinusoidal blood capillaries were further sub-classified as non-fenestrated or fenestrated based on the absence or presence of endothelial cells with fenestrations. The sinusoidal blood capillaries of the liver, myeloid (red) bone marrow, and spleen were sub-classified as reticuloendothelial or non-reticuloendothelial based on the phago-endocytic capacity of the endothelial cells.
The physiologic upper limit of pore size for transvascular flow across capillary walls of non-sinusoidal non-fenestrated blood capillaries is less than 1 nm for those with interendothelial cell clefts lined with zona occludens junctions (i.e. brain and spinal cord), and approximately 5 nm for those with clefts lined with macula occludens junctions (i.e. skeletal muscle). The physiologic upper limit of pore size for transvascular flow across the capillary walls of non-sinusoidal fenestrated blood capillaries with diaphragmed fenestrae ranges between 6 and 12 nm (i.e. exocrine and endocrine glands); whereas, the physiologic upper limit of pore size for transvascular flow across the capillary walls of non-sinusoidal fenestrated capillaries with open 'non-diaphragmed' fenestrae is approximately 15 nm (kidney glomerulus). In the case of the sinusoidal reticuloendothelial blood capillaries of myeloid bone marrow, the transvascular transport of non-endogenous macromolecules larger than 5 nm into the bone marrow interstitial space takes place via reticuloendothelial cell-mediated phago-endocytosis and transvascular release, which is the case for systemic bone marrow imaging agents as large as 60 nm in diameter.
The physiologic upper limit of pore size in the capillary walls of most non-sinusoidal blood capillaries to the transcapillary passage of lipid-insoluble endogenous and non-endogenous macromolecules ranges between 5 and 12 nm. Therefore, macromolecules larger than the physiologic upper limits of pore size in the non-sinusoidal blood capillary types generally do not accumulate within the respective tissue interstitial spaces and their lymphatic drainages. In the case of reticuloendothelial sinusoidal blood capillaries of myeloid bone marrow, however, non-endogenous macromolecules as large as 60 nm in diameter can distribute into the bone marrow interstitial space via the phago-endocytic route, and then subsequently accumulate in the locoregional lymphatic drainages of tissues following absorption into the lymphatic drainage of periosteal fibrous tissues, which is the lymphatic drainage of myeloid bone marrow. When the ultrastructural basis for transcapillary exchange across the capillary walls of different capillary types is viewed in this light, it becomes evident that the physiologic evidence for the existence of aqueous large pores ranging between 24 and 60 nm in diameter in the capillary walls of blood capillaries, is circumstantial, at best.
我们目前对微血管通透性的许多理解是基于对毛细血管对各种大小的脂溶性内源性和非内源性大分子通透性的经典实验研究结果。根据基于对各种大小的全身或局部灌注内源性大分子跨毛细血管流速研究结果制定的经典微血管通透性小孔理论,跨毛细血管壁的跨毛细血管交换通过单一群体的直径约为6nm的小孔进行;而根据基于对各种大小的全身或局部灌注非内源性大分子在局部组织淋巴引流中积累的研究结果制定的微血管通透性双孔理论,跨毛细血管壁的跨毛细血管交换也通过另一群体的直径在24至60nm之间的大孔或毛细血管渗漏进行。基于跨血管流动的孔径生理上限差异对毛细血管类型进行分类,突出了内源性和非内源性大分子跨不同类型毛细血管壁进行跨血管运输的跨毛细血管交换途径的差异。
回顾了20世纪50年代至今关于毛细血管壁超微结构以及毛细血管对脂溶性内源性和非内源性分子微血管通透性的研究结果和已发表数据。在本研究中,根据脂溶性分子跨血管流动的孔径生理上限对不同组织和器官中的毛细血管类型进行分类。根据毛细血管壁基底膜层的连续性与否,将毛细血管分为非窦状或窦状。非窦状毛细血管根据有无有窗孔的内皮细胞进一步细分为无窗孔或有窗孔。肝脏、骨髓(红)和脾脏的窦状毛细血管根据内皮细胞的吞噬内吞能力细分为网状内皮或非网状内皮。
对于内皮细胞间裂由紧密连接排列的非窦状无窗孔毛细血管(即脑和脊髓),跨毛细血管壁跨血管流动的孔径生理上限小于1nm;对于裂由闭锁小带排列的(即骨骼肌),约为5nm。对于有隔膜窗孔的非窦状有窗孔毛细血管壁,跨血管流动的孔径生理上限在6至12nm之间(即外分泌和内分泌腺);而对于有开放“无隔膜”窗孔的非窦状有窗孔毛细血管壁,跨血管流动的孔径生理上限约为15nm(肾小球)。在骨髓的窦状网状内皮毛细血管中,大于5nm的非内源性大分子跨血管运输到骨髓间质空间是通过网状内皮细胞介导的吞噬内吞和跨血管释放进行的,直径达60nm的全身骨髓显像剂就是这种情况。
大多数非窦状毛细血管壁对脂溶性内源性和非内源性大分子跨毛细血管通道的孔径生理上限在5至12nm之间。因此,大于非窦状毛细血管类型孔径生理上限的大分子通常不会在各自的组织间质空间及其淋巴引流中积累。然而,在骨髓的网状内皮窦状毛细血管中,直径达60nm的非内源性大分子可通过吞噬内吞途径分布到骨髓间质空间,然后在被骨膜纤维组织的淋巴引流(即骨髓的淋巴引流)吸收后,随后在局部组织淋巴引流中积累。当从这个角度看待不同类型毛细血管壁跨毛细血管交换的超微结构基础时,很明显,关于在毛细血管壁中存在直径在24至60nm之间的水性大孔的生理证据,充其量只是间接的。