Institute for Clinical Evaluative Sciences, Toronto, Ontario, Canada.
PLoS One. 2010 Aug 13;5(8):e12150. doi: 10.1371/journal.pone.0012150.
Survivors of anterior MI are at increased risk for stroke with predilection to form ventricular thrombus. Commonly patients are discharged on dual antiplatelet therapy. Given the frequency of early coronary reperfusion and risk of bleeding, it remains uncertain whether anticoagulation offers additional utility. We examined the effectiveness of anticoagulation therapy for the prevention of stroke after anterior MI.
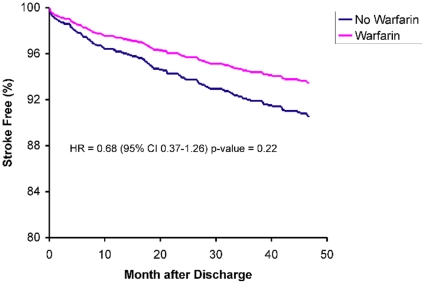
We performed a population-based cohort analysis of 10,383 patients who survived hospitalization for an acute MI in Ontario, Canada from April 1, 1999 to March 31, 2001. The primary outcome was four-year ischemic stroke rates compared between anterior and non-anterior MI patients. Risk factors for stroke were assessed by multivariate Cox proportional-hazards analysis. Warfarin use was determined at discharge and followed for 90 days among a subset of patients aged 66 and older (n = 1483). Among the 10,383 patients studied, 2,942 patients survived hospitalization for an anterior MI and 20% were discharged on anticoagulation therapy. Within 4 years, 169 patients (5.7%) were admitted with an ischemic stroke, half of which occurred within 1-year post-MI. There was no significant difference in stroke rate between anterior and non-anterior MI patients. The use of warfarin up to 90 days was not associated with stroke protection after anterior MI (hazard ratio [HR], 0.68; 95% confidence interval [CI], 0.37-1.26). The use of angiotensin-converting-enzyme inhibitors (HR, 0.65; 95% CI, 0.44-0.95) and beta-blockers (HR, 0.60; 95% CI, 0.41-0.87) were associated with a significant decrease in stroke risk. There was no significant difference in bleeding-related hospitalizations in patients who used warfarin for up to 90 days post-MI.
Many practitioners still consider a large anterior-wall MI as high risk for potential LV thrombus formation and stroke. Among a cohort of elderly patients who survived an anterior MI there was no benefit from the use of warfarin up to 90 days post-MI to prevent ischemic stroke. Our data suggests that routine anticoagulation of patients with anterior-wall MI may not be indicated. Prospective randomized trials are needed to determine the optimal antithrombin strategy for preventing this common and serious adverse outcome.
前壁心肌梗死幸存者发生中风的风险增加,且易形成心室血栓。通常患者出院时接受双联抗血小板治疗。鉴于早期冠状动脉再灌注的频率和出血风险,抗凝治疗是否提供额外益处仍不确定。我们研究了抗凝治疗在前壁心肌梗死后预防中风的效果。
我们对 1999 年 4 月 1 日至 2001 年 3 月 31 日期间在加拿大安大略省因急性心肌梗死住院存活的 10383 例患者进行了基于人群的队列分析。主要结局是比较前壁和非前壁心肌梗死患者的四年缺血性中风发生率。采用多变量 Cox 比例风险分析评估中风的危险因素。在年龄在 66 岁及以上的亚组患者中(n=1483),出院时确定华法林的使用情况并随访 90 天。在研究的 10383 例患者中,2942 例患者存活住院治疗前壁心肌梗死,20%的患者出院时接受抗凝治疗。在 4 年内,169 例患者(5.7%)因缺血性中风入院,其中一半发生在心肌梗死后 1 年内。前壁和非前壁心肌梗死患者的中风发生率无显著差异。在接受前壁心肌梗死后的 90 天内使用华法林与中风保护无关(风险比[HR],0.68;95%置信区间[CI],0.37-1.26)。使用血管紧张素转换酶抑制剂(HR,0.65;95%CI,0.44-0.95)和β受体阻滞剂(HR,0.60;95%CI,0.41-0.87)与中风风险显著降低相关。在接受前壁心肌梗死后 90 天内使用华法林的患者中,与出血相关的住院治疗无显著差异。
许多医生仍认为大面积前壁心肌梗死易形成潜在的左心室血栓形成和中风。在前壁心肌梗死存活的老年患者队列中,在前壁心肌梗死后 90 天内使用华法林预防缺血性中风并无获益。我们的数据表明,常规抗凝治疗大面积前壁心肌梗死可能没有必要。需要进行前瞻性随机试验来确定预防这种常见且严重不良结局的最佳抗血栓策略。