Department of Emergency Medicine, University of Pittsburgh, Pittsburgh, PA, USA.
Prehosp Emerg Care. 2010 Oct-Dec;14(4):413-8. doi: 10.3109/10903127.2010.497902.
Return of spontaneous circulation (ROSC) occurs in 35.0 to 61.0% of emergency medical services (EMS)-treated out-of-hospital cardiac arrests (OHCAs); however, not all patients achieving ROSC survive to hospital arrival or discharge. Previous studies have estimated the incidence of some types of rearrest(RA) at 61.0 to 79.0%, and the electrocardiogram (ECG) waveform characteristics of prehospital RA rhythms have not been previously described.
We sought to determine the incidence of RA in OHCA, to classify RA events by type, and to measure the time from ROSC to RA. We also conducted a preliminary analysis of the relationship between first EMS-detected rhythms and RA, as well as the effect of RA on survival.
The Pittsburgh Regional Clinical Center of the National Heart, Lung, and Blood Institute (NHLBI) -sponsored Resuscitation Outcomes Consortium (ROC) provided cases from a population-based cardiac arrest surveillance program, ROC Epistry. Only OHCA cases of nontraumatic etiology with available and adequate ECG files were included. We analyzed defibrillator-monitor ECG tracings (Philips MRX), patient care reports (PCRs), and defibrillator audio recordings from EMS-treated cases of OHCA spanning the period from October 2006 to December 2008. We identified ROSC and RA through interpretation of ECG tracings and audio recordings. Rearrest events were categorized as ventricular fibrillation (VF), pulseless ventricular tachycardia (VT), asystole, and pulseless electrical activity (PEA) based on ECG waveform characteristics. Proportions of RA rhythms were stratified by first EMS rhythm and compared using Pearson's chi-square test. Logistic regression was used to test the predictive relationship between RA and survival to hospital discharge.
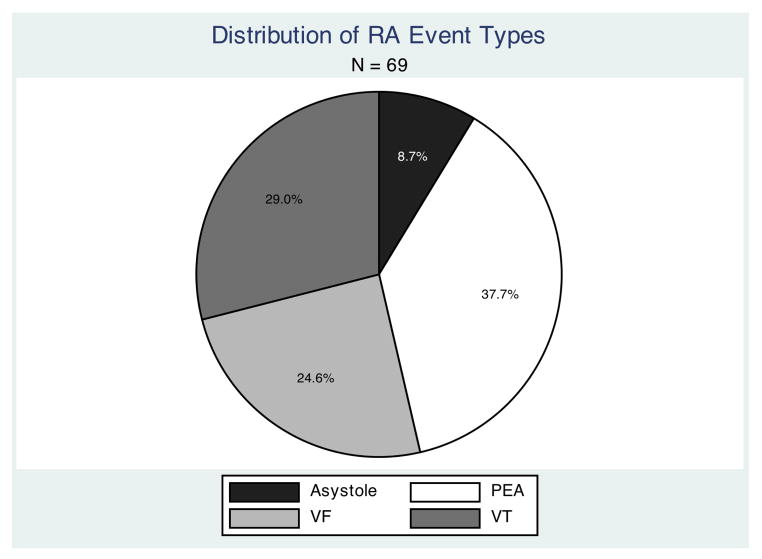
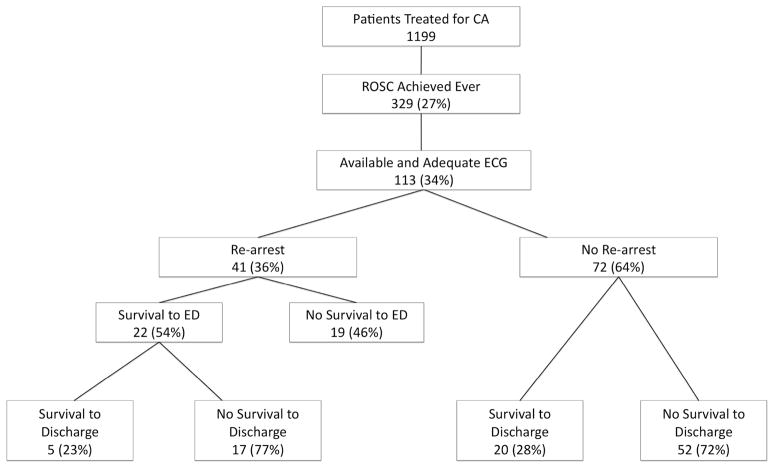
Return of spontaneous circulation occurred in 329 of 1,199 patients (27.4% [95.0% confidence interval (CI): 25.0-30.0%]) treated for cardiac arrest. Of these, 113 had ECG tracings that were available and adequate for analysis. Rearrest occurred in 41 patients (36.0% [95.0% CI: 26.0-46.0%]), with a total of 69 RA events. Survival to hospital discharge in RA cases was 23.1% (95.0% CI: 11.1-39.3%), compared with 27.8% (95.0% CI: 17.9-39.6%) in cases without RA. Counts of RA events by type were as follows: 17 VF (24.6% [95% CI: 15.2-36.5%]), 20 pulseless VT (29.0% [95.0% CI: 18.7-41.2%]), 26 PEA (37.0% [95.0% CI: 26.3-50.2%]), and six asystole (8.8% [95.0% CI: 3.3-18.0%]). Rearrest was not predictive of survival to hospital discharge; however, initial EMS rhythm was predictive of RA shockability. The overall median (interquartile range) time from ROSC to RA among all events was 3.1 (1.6-6.3) minutes.
In this sample, the incidence of RA was 38.0%. The most common type of RA was PEA. Shockability of first EMS rhythm was found to predict subsequent RA rhythm shockability.
在接受紧急医疗服务(EMS)治疗的院外心脏骤停(OHCA)患者中,有 35.0%至 61.0%出现自主循环恢复(ROSC);然而,并非所有 ROSC 患者都能存活至医院到达或出院。先前的研究估计某些类型的再逮捕(RA)的发生率为 61.0%至 79.0%,并且先前没有描述过院前 RA 节律的心电图(ECG)波形特征。
我们旨在确定 OHCA 中的 RA 发生率,通过类型对 RA 事件进行分类,并测量从 ROSC 到 RA 的时间。我们还对首次 EMS 检测到的节律与 RA 之间的关系以及 RA 对生存率的影响进行了初步分析。
国家心肺血液研究所(NHLBI)赞助的复苏结果联合会(ROC)的匹兹堡地区临床中心从基于人群的心脏骤停监测计划 ROC Epistry 中提供了病例。仅包括具有可用且足够的 ECG 文件的非创伤性病因的 OHCA 病例。我们分析了来自 EMS 治疗的 OHCA 病例的除颤监护仪 ECG 轨迹(飞利浦 MRX)、患者护理报告(PCR)和除颤器音频记录。通过 ECG 轨迹和音频记录的解释来识别 ROSC 和 RA。根据 ECG 波形特征,将 RA 事件归类为心室颤动(VF)、无脉搏性室性心动过速(VT)、心搏停止和无脉搏性电活动(PEA)。按首次 EMS 节律对 RA 节律的比例进行分层,并使用 Pearson 卡方检验进行比较。使用逻辑回归检验 RA 与医院出院存活率之间的预测关系。
在接受心脏骤停治疗的 1199 名患者中,有 329 名患者(27.4%[95.0%置信区间(CI):25.0-30.0%])出现 ROSC。其中,有 113 名患者有可用且足够分析的 ECG 轨迹。在 41 名患者(36.0%[95.0%CI:26.0-46.0%])中发生了 RA,总共发生了 69 次 RA 事件。RA 病例的存活率为 23.1%(95.0%CI:11.1-39.3%),而无 RA 病例的存活率为 27.8%(95.0%CI:17.9-39.6%)。按类型划分的 RA 事件计数如下:17 例 VF(24.6%[95%CI:15.2-36.5%])、20 例无脉搏 VT(29.0%[95.0%CI:18.7-41.2%])、26 例 PEA(37.0%[95.0%CI:26.3-50.2%])和 6 例心搏停止(8.8%[95.0%CI:3.3-18.0%])。RA 与医院出院存活率无关;然而,初始 EMS 节律与 RA 可电击性相关。所有事件中从 ROSC 到 RA 的中位(四分位距)时间为 3.1(1.6-6.3)分钟。
在本样本中,RA 的发生率为 38.0%。最常见的 RA 类型是 PEA。首次 EMS 节律的可电击性预测了随后的 RA 节律可电击性。