Medical School, University of Tampere, Finland.
Acta Orthop. 2010 Aug;81(4):413-9. doi: 10.3109/17453674.2010.501747.
Total knee replacements (TKRs) are being increasingly performed in patients aged < or = 65 years who often have high physical demands. We investigated the relation between age of the patient and prosthesis survival following primary TKR using nationwide data collected from the Finnish Arthroplasty Register.
From Jan 1, 1997 through Dec 31, 2003, 32,019 TKRs for primary or secondary osteoarthritis were reported to the Finnish Arthroplasty Register. The TKRs were followed until the end of 2004. During the follow-up, 909 TKRs were revised, 205 (23%) due to infection and 704 for other reasons.
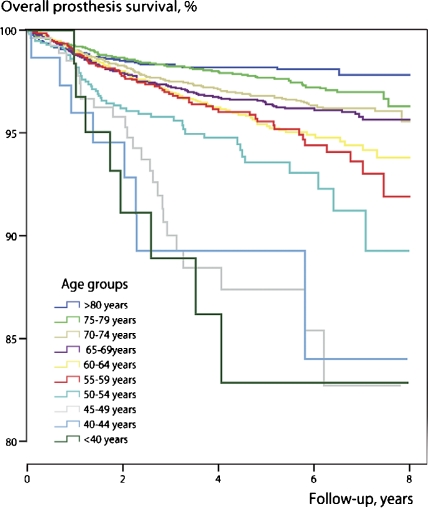
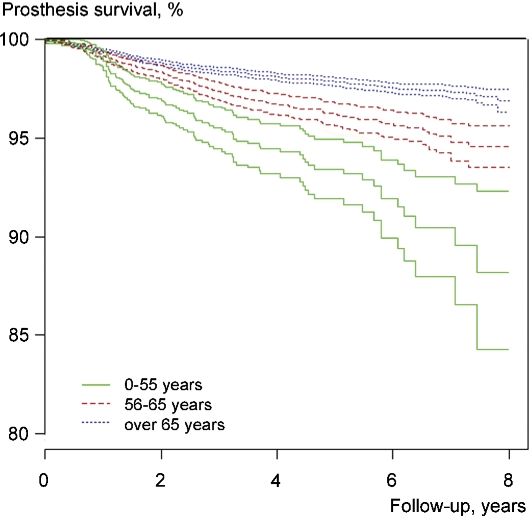
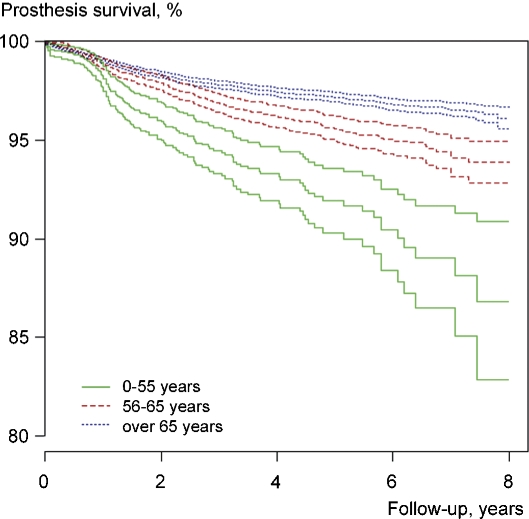
Crude overall implant survival improved with increasing age between the ages of 40 and 80. The 5-year survival rates were 92% and 95% in patients aged < or = 55 and 56-65 years, respectively, compared to 97% in patients who were > 65 years of age (p < 0.001). The difference was mainly attributable to reasons other than infections. Sex, diagnosis, type of TKR (condylar, constrained, or hinge), use of patellar component, and fixation method were also associated with higher revision rates. However, the differences in prosthesis survival between the age groups < or = 55, 56-65, and > 65 years remained after adjustment for these factors (p < 0.001).
Young age impairs the prognosis of TKR and is associated with increased revision rates for non-infectious reasons. Diagnosis, sex, type of TKR, use of patellar component, and fixation method partly explain the differences, but the effects of physical activity, patient demands, and obesity on implant survival in younger patients warrant further research.
在年龄≤65 岁、身体活动需求较高的患者中,全膝关节置换术(TKR)的应用日益增多。我们利用来自芬兰关节置换登记处的全国性数据,研究了患者年龄与初次 TKR 后假体生存率之间的关系。
1997 年 1 月 1 日至 2003 年 12 月 31 日,共有 32019 例 TKR 用于原发性或继发性骨关节炎,向芬兰关节置换登记处报告。TKR 随访至 2004 年底。随访期间,909 例 TKR 进行了翻修,205 例(23%)因感染,704 例因其他原因。
在 40-80 岁的年龄段内,总体植入物的粗存活率随年龄的增加而提高。<55 岁和 56-65 岁的患者 5 年生存率分别为 92%和 95%,而>65 岁的患者为 97%(p<0.001)。这种差异主要归因于感染以外的其他原因。性别、诊断、TKR 类型(髁间、约束、铰链)、髌骨组件的使用和固定方法也与较高的翻修率相关。然而,在调整这些因素后,<55 岁、56-65 岁和>65 岁年龄组之间的假体生存率差异仍然存在(p<0.001)。
年轻的年龄会影响 TKR 的预后,并与非感染性原因的翻修率增加相关。诊断、性别、TKR 类型、髌骨组件的使用和固定方法部分解释了这些差异,但身体活动、患者需求和肥胖对年轻患者植入物生存率的影响仍需进一步研究。