Department of Orthopedic Surgery, Aarhus University Hospital, Aarhus, Denmark.
Acta Orthop. 2010 Oct;81(5):606-10. doi: 10.3109/17453674.2010.519165.
There have been few studies describing wound infiltration with additional intraarticular administration of multimodal analgesia for total knee arthroplasty (TKA). In this study, we assessed the efficacy of wound infiltration combined with intraarticular regional analgesia with epidural infusion on analgesic requirements and postoperative pain after TKA.
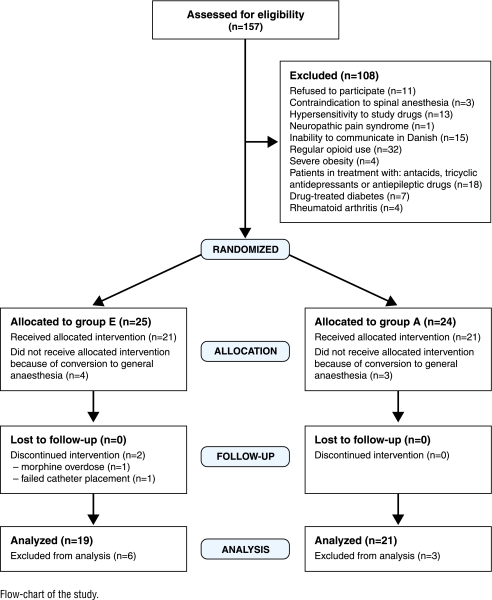
40 consecutive patients undergoing elective, primary TKA were randomized into 2 groups to receive either (1) intraoperative wound infiltration with 150 mL ropivacaine (2 mg/mL), 1 mL ketorolac (30 mg/mL), and 0.5 mL epinephrine (1 mg/mL) (total volume 152 mL) combined with intraarticular infusion (4 mL/h) of 190 mL ropivacaine (2 mg/mL) plus 2 mL ketorolac (30 mg/mL) (group A), or (2) epidural infusion (4 mL/h) of 192 mL ropivacaine (2 mg/mL) combined with 6 intravenous administrations of 0.5 mL ketorolac (30 mg/mL) for 48 h postoperatively (group E). For rescue analgesia, intravenous patient-controlled-analgesia (PCA) morphine was used. Morphine consumption, intensity of knee pain (0–100 mm visual analog scale), and side effects were recorded. Length of stay and corrected length of stay were also recorded (the day-patients fulfilled discharge criteria).
The median cumulated morphine consumption, pain scores at rest, and pain scores during mobilization were reduced in group A compared to group E. Corrected length of stay was reduced by 25% in group A compared to group E.
Peri- and intraarticular analgesia with multimodal drugs provided superior pain relief and reduced morphine consumption compared with continuous epidural infusion with ropivacaine combined with intravenous ketorolac after TKA.
对于全膝关节置换术(TKA),仅有少数研究描述了在伤口浸润的基础上联合关节内注射多模式镇痛的效果。本研究旨在评估 TKA 术后伤口浸润联合关节内区域性镇痛与硬膜外输注的镇痛效果和术后疼痛情况。
连续纳入 40 例行择期初次 TKA 的患者,随机分为两组:(1)术中伤口浸润 150 mL 罗哌卡因(2 mg/mL)、1 mL 酮咯酸(30 mg/mL)和 0.5 mL 肾上腺素(1 mg/mL)(总体积 152 mL),联合关节内输注 190 mL 罗哌卡因(2 mg/mL)加 2 mL 酮咯酸(30 mg/mL)(4 mL/h)(A 组),或(2)硬膜外输注(4 mL/h)192 mL 罗哌卡因(2 mg/mL),联合术后 48 小时内静脉注射 6 次 0.5 mL 酮咯酸(30 mg/mL)(E 组)。用于解救性镇痛的药物为静脉患者自控镇痛(PCA)吗啡。记录吗啡用量、膝关节疼痛强度(0-100mm 视觉模拟评分)和不良反应。还记录了住院时间和校正住院时间(患者满足出院标准的天数)。
与 E 组相比,A 组的累积吗啡用量、静息时疼痛评分和活动时疼痛评分中位数均降低。与 E 组相比,A 组的校正住院时间减少了 25%。
与 TKA 后持续硬膜外输注罗哌卡因联合静脉酮咯酸相比,多模式药物围手术期和关节内镇痛可提供更好的疼痛缓解,并减少吗啡用量。