National Surgical Adjuvant Breast and Bowel Project (NSABP), Pittsburgh, PA, USA.
Lancet Oncol. 2010 Oct;11(10):927-33. doi: 10.1016/S1470-2045(10)70207-2.
Sentinel-lymph-node (SLN) surgery was designed to minimise the side-effects of lymph-node surgery but still offer outcomes equivalent to axillary-lymph-node dissection (ALND). The aims of National Surgical Adjuvant Breast and Bowel Project (NSABP) trial B-32 were to establish whether SLN resection in patients with breast cancer achieves the same survival and regional control as ALND, but with fewer side-effects.
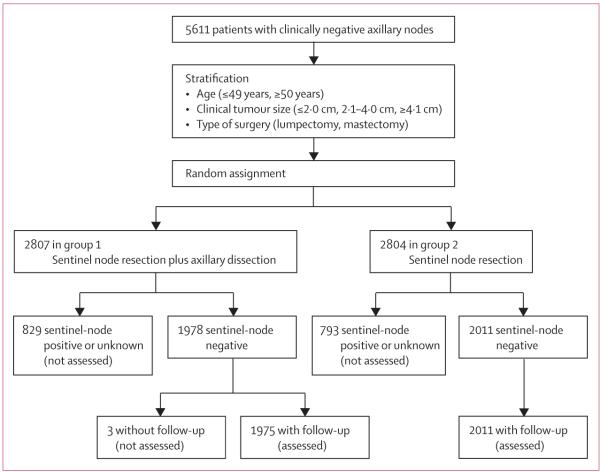
NSABP B-32 was a randomised controlled phase 3 trial done at 80 centres in Canada and the USA between May 1, 1999, and Feb 29, 2004. Women with invasive breast cancer were randomly assigned to either SLN resection plus ALND (group 1) or to SLN resection alone with ALND only if the SLNs were positive (group 2). Random assignment was done at the NSABP Biostatistical Center (Pittsburgh, PA, USA) with a biased coin minimisation approach in an allocation ratio of 1:1. Stratification variables were age at entry (≤ 49 years, ≥ 50 years), clinical tumour size (≤ 2·0 cm, 2·1-4·0 cm, ≥ 4·1 cm), and surgical plan (lumpectomy, mastectomy). SLN resection was done with a blue dye and radioactive tracer. Outcome analyses were done in patients who were assessed as having pathologically negative sentinel nodes and for whom follow-up data were available. The primary endpoint was overall survival. Analyses were done on an intention-to-treat basis. All deaths, irrespective of cause, were included. The mean time on study for the SLN-negative patients with follow-up information was 95·6 months (range 70·1-126·7). This study is registered with ClinicalTrials.gov, number NCT00003830.
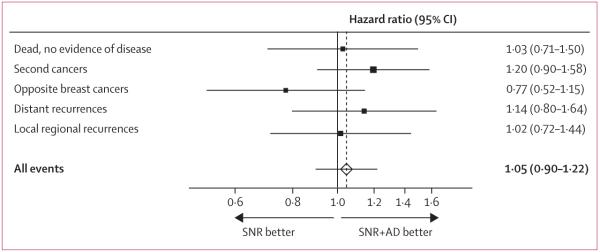
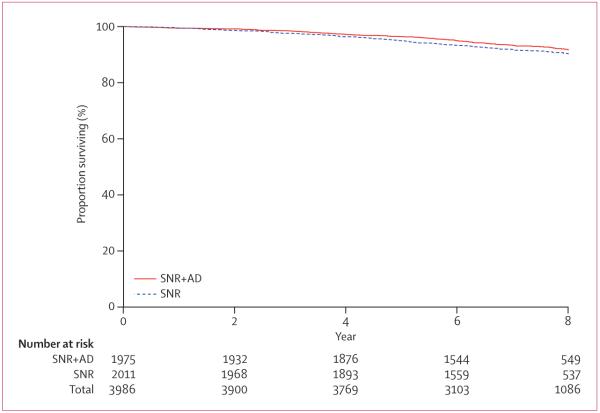
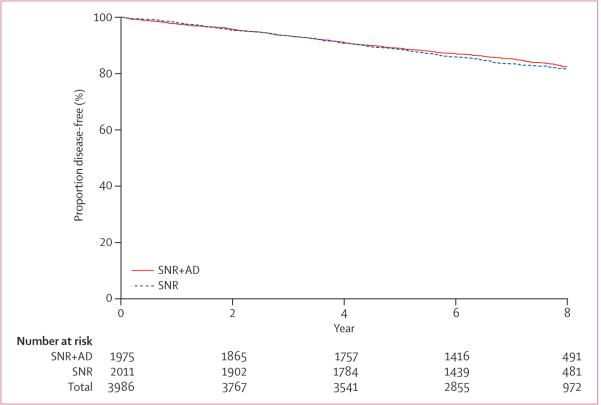
5611 women were randomly assigned to the treatment groups, 3989 had pathologically negative SLN. 309 deaths were reported in the 3986 SLN-negative patients with follow-up information: 140 of 1975 patients in group 1 and 169 of 2011 in group 2. Log-rank comparison of overall survival in groups 1 and 2 yielded an unadjusted hazard ratio (HR) of 1·20 (95% CI 0·96-1·50; p=0·12). 8-year Kaplan-Meier estimates for overall survival were 91·8% (95% CI 90·4-93·3) in group 1 and 90·3% (88·8-91·8) in group 2. Treatment comparisons for disease-free survival yielded an unadjusted HR of 1·05 (95% CI 0·90-1·22; p=0·54). 8-year Kaplan-Meier estimates for disease-free survival were 82·4% (80·5-84·4) in group 1 and 81·5% (79·6-83·4) in group 2. There were eight regional-node recurrences as first events in group 1 and 14 in group 2 (p=0·22). Patients are continuing follow-up for longer-term assessment of survival and regional control. The most common adverse events were allergic reactions, mostly related to the administration of the blue dye.
Overall survival, disease-free survival, and regional control were statistically equivalent between groups. When the SLN is negative, SLN surgery alone with no further ALND is an appropriate, safe, and effective therapy for breast cancer patients with clinically negative lymph nodes.
US Public Health Service, National Cancer Institute, and Department of Health and Human Services.
前哨淋巴结(SLN)手术旨在最大限度地减少淋巴结手术的副作用,但仍能提供与腋窝淋巴结清扫术(ALND)相当的结果。国家外科辅助乳腺和肠道项目(NSABP)B-32 试验的目的是确定乳腺癌患者的 SLN 切除术是否与 ALND 一样具有相同的生存率和局部控制率,但副作用更少。
NSABP B-32 是一项在加拿大和美国的 80 个中心进行的随机对照 3 期试验,于 1999 年 5 月 1 日至 2004 年 2 月 29 日进行。浸润性乳腺癌患者被随机分配到 SLN 切除术加 ALND(组 1)或 SLN 切除术加 ALND,仅当 SLN 阳性时(组 2)。随机分配由匹兹堡 NSABP 生物统计学中心(美国宾夕法尼亚州)进行,采用偏倚硬币最小化方法,分配比例为 1:1。分层变量为年龄(≤49 岁,≥50 岁)、临床肿瘤大小(≤2.0cm,2.1-4.0cm,≥4.1cm)和手术计划(乳房切除术,乳房切除术)。SLN 切除术采用蓝色染料和放射性示踪剂进行。对病理上评估为 SLN 阴性且有随访数据的患者进行结果分析。主要终点是总生存率。分析采用意向治疗。所有死亡,无论原因如何,均包括在内。有随访信息的 SLN 阴性患者的平均研究时间为 95.6 个月(70.1-126.7)。本研究在 ClinicalTrials.gov 注册,编号为 NCT00003830。
5611 名女性被随机分配到治疗组,3989 名女性的 SLN 呈病理阴性。在有随访信息的 3986 名 SLN 阴性患者中报告了 309 例死亡:组 1 中有 1975 例中的 140 例,组 2 中有 2011 例中的 169 例。对组 1 和组 2 的总生存率进行对数秩比较,得出未调整的危险比(HR)为 1.20(95%CI 0.96-1.50;p=0.12)。组 1 的 8 年 Kaplan-Meier 总生存率估计值为 91.8%(95%CI 90.4-93.3),组 2 为 90.3%(88.8-91.8)。无病生存率的治疗比较得出未调整的 HR 为 1.05(95%CI 0.90-1.22;p=0.54)。组 1 的 8 年 Kaplan-Meier 无病生存率估计值为 82.4%(80.5-84.4),组 2 为 81.5%(79.6-83.4)。组 1 中有 8 例局部淋巴结复发作为首发事件,组 2 中有 14 例(p=0.22)。患者正在继续进行长期生存和局部控制评估。最常见的不良事件是过敏反应,主要与蓝色染料的给药有关。
总生存率、无病生存率和局部控制率在两组之间统计学上等效。当 SLN 为阴性时,单独进行 SLN 切除术而不进一步进行 ALND 是一种合适、安全和有效的治疗方法,适用于临床淋巴结阴性的乳腺癌患者。
美国公共卫生服务部、美国国家癌症研究所和美国卫生与公众服务部。