Centre for International Health and Development, UCL Institute of Child Health, 30 Guilford Street, London WC1N 1EH, UK.
Arch Dis Child. 2010 Dec;95(12):1039-46. doi: 10.1136/adc.2009.179366. Epub 2010 Oct 26.
Perinatal conditions make the largest contribution to the burden of disease in low-income countries. Although postneonatal mortality rates have declined, stillbirth and early neonatal mortality rates remain high in many countries in Africa and Asia, and there is a concentration of mortality around the time of birth. Our article begins by considering differences in the interpretation of 'intervention' to improve perinatal survival. We identify three types of
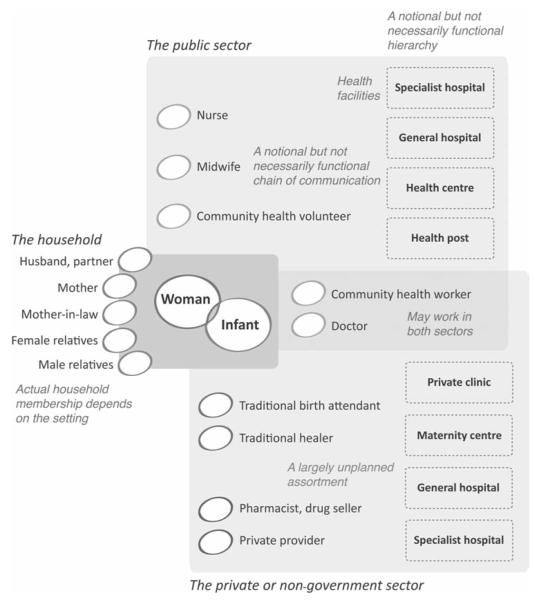
a single action, a collection of actions delivered in a package and a broader social or system approach. We use this classification to summarise the findings of recent systematic reviews and meta-analyses. After describing the growing evidence base for the effectiveness of community-based perinatal care, we discuss current concerns about integration: of women's and children's health programmes, of community-based and institutional care, and of formal and informal sector human resources. We end with some thoughts on the complexity of choices confronting women and their families in low-income countries, particularly in view of the growth in non-government and private sector healthcare.
围产期状况是低收入国家疾病负担的最大成因。尽管新生后死亡率有所下降,但在非洲和亚洲的许多国家,死产和早期新生儿死亡率仍然很高,而且死亡集中在分娩前后。我们的文章首先考虑了改善围产儿生存的“干预措施”的不同解释。我们确定了三种干预措施:单项行动、一整套行动以及更广泛的社会或系统方法。我们使用这种分类来总结最近系统评价和荟萃分析的结果。在描述了以社区为基础的围产保健有效性日益增多的证据之后,我们讨论了目前对整合的关切:妇女和儿童保健方案的整合、以社区为基础的和机构的保健的整合以及正规和非正规部门人力资源的整合。最后,我们对低收入国家妇女及其家庭所面临的选择的复杂性进行了思考,尤其是鉴于非政府和私营部门保健的增长。