Department of Anaesthesiology and Critical Care Medicine, Estaing Hospital, University Hospital of Clermont-Ferrand, 1 Place Lucie Aubrac, Clermont-Ferrand, 63000, France.
Crit Care. 2010;14(5):R193. doi: 10.1186/cc9310. Epub 2010 Oct 29.
Central venous oxygen saturation (ScvO2) is a useful therapeutic target in septic shock and high-risk surgery. We tested the hypothesis that central venous-to-arterial carbon dioxide difference (P(cv-a)CO2), a global index of tissue perfusion, could be used as a complementary tool to ScvO2 for goal-directed fluid therapy (GDT) to identify persistent low flow after optimization of preload has been achieved by fluid loading during high-risk surgery.
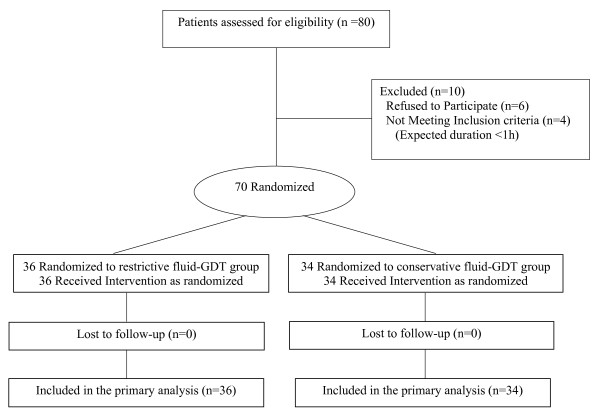
This is a secondary analysis of results obtained in a study involving 70 adult patients (ASA I to III), undergoing major abdominal surgery, and treated with an individualized goal-directed fluid replacement therapy. All patients were managed to maintain a respiratory variation in peak aortic flow velocity below 13%. Cardiac index (CI), oxygen delivery index (DO2i), ScvO2, P(cv-a)CO2 and postoperative complications were recorded blindly for all patients.
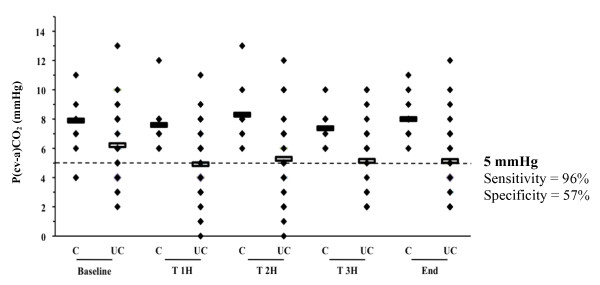
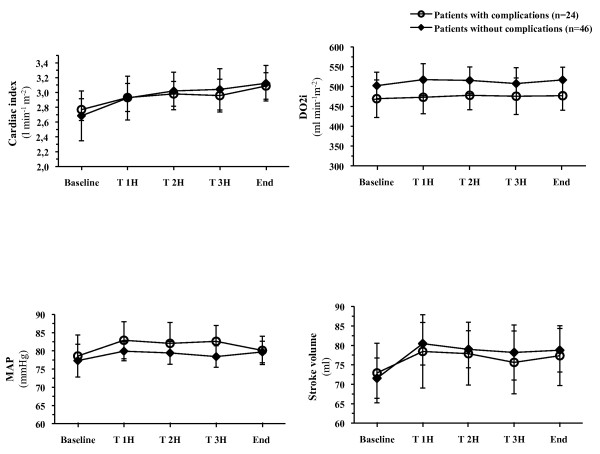
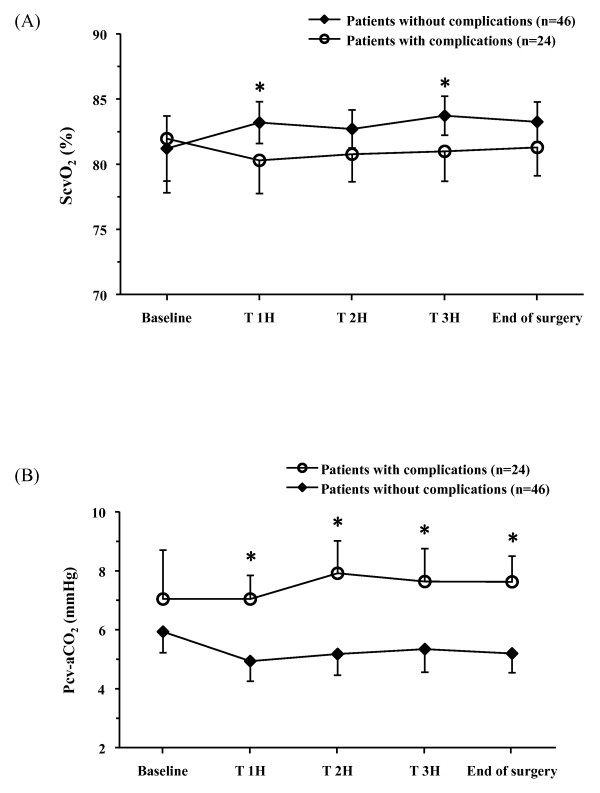
A total of 34% of patients developed postoperative complications. At baseline, there was no difference in demographic or haemodynamic variables between patients who developed complications and those who did not. In patients with complications, during surgery, both mean ScvO2 (78 ± 4 versus 81 ± 4%, P = 0.017) and minimal ScvO2 (minScvO2) (67 ± 6 versus 72 ± 6%, P = 0.0017) were lower than in patients without complications, despite perfusion of similar volumes of fluids and comparable CI and DO2i values. The optimal ScvO2 cut-off value was 70.6% and minScvO2 < 70% was independently associated with the development of postoperative complications (OR = 4.2 (95% CI: 1.1 to 14.4), P = 0.025). P(cv-a)CO2 was larger in patients with complications (7.8 ± 2 versus 5.6 ± 2 mmHg, P < 10-6). In patients with complications and ScvO2 ≥ 71%, P(cv-a)CO2 was also significantly larger (7.7 ± 2 versus 5.5 ± 2 mmHg, P < 10-6) than in patients without complications. The area under the receiver operating characteristic (ROC) curve was 0.785 (95% CI: 0.74 to 0.83) for discrimination of patients with ScvO2 ≥ 71% who did and did not develop complications, with 5 mmHg as the most predictive threshold value.
ScvO2 reflects important changes in O2 delivery in relation to O2 needs during the perioperative period. A P(cv-a)CO2 < 5 mmHg might serve as a complementary target to ScvO2 during GDT to identify persistent inadequacy of the circulatory response in face of metabolic requirements when an ScvO2 ≥ 71% is achieved.
Clinicaltrials.gov Identifier: NCT00852449.
中心静脉血氧饱和度(ScvO2)是脓毒症休克和高危手术中有用的治疗目标。我们检验了这样一个假设,即中心静脉-动脉二氧化碳分压差(P(cv-a)CO2),作为组织灌注的一个整体指标,可以作为 ScvO2 的补充工具,用于目标导向的液体治疗(GDT),以确定在高危手术中通过液体负荷优化前负荷后仍存在持续低流量。
这是一项涉及 70 名接受大腹部手术的成年患者(ASA I 至 III 级)的研究结果的二次分析,这些患者接受了个体化的目标导向液体替代治疗。所有患者均接受治疗以维持主动脉峰值血流速度的呼吸变异低于 13%。所有患者均记录了心指数(CI)、氧输送指数(DO2i)、ScvO2、P(cv-a)CO2 和术后并发症。
共有 34%的患者发生了术后并发症。在基线时,发生并发症的患者与未发生并发症的患者在人口统计学和血流动力学变量方面无差异。在发生并发症的患者中,尽管输注了相似的液体量,并且 CI 和 DO2i 值相当,但术中平均 ScvO2(78±4%比 81±4%,P=0.017)和最小 ScvO2(minScvO2)(67±6%比 72±6%,P=0.0017)均较低。最佳 ScvO2 截断值为 70.6%,minScvO2<70%与术后并发症的发生独立相关(OR=4.2(95%CI:1.1 至 14.4),P=0.025)。发生并发症的患者 P(cv-a)CO2 较大(7.8±2比 5.6±2mmHg,P<10-6)。在发生并发症且 ScvO2≥71%的患者中,P(cv-a)CO2 也明显更大(7.7±2比 5.5±2mmHg,P<10-6)。接受者操作特征(ROC)曲线下面积为 0.785(95%CI:0.74 至 0.83),用于区分 ScvO2≥71%的患者是否发生并发症,5mmHg 为最具预测性的阈值。
ScvO2 反映了围手术期 O2 输送与 O2 需求之间的重要变化。当 ScvO2≥71%时,P(cv-a)CO2<5mmHg 可能是 GDT 的一个补充目标,以在代谢需求存在的情况下识别循环反应持续不足,从而避免循环反应不足。
Clinicaltrials.gov 标识符:NCT00852449。