Service d'Anesthésie Réanimation Chirurgicale, DMU 12 Anesthésie Réanimation Chirurgicale Médecine Péri-Opératoire et Douleur, Hôpital Bicêtre, AP-HP, Université Paris-Saclay, Équipe DYNAMIC, Inserm UMR_S999, Le Kremlin-Bicêtre, France.
Service d'Anesthésie Réanimation Chirurgicale, DMU 12 Anesthésie Réanimation Chirurgicale Médecine Péri-Opératoire et Douleur, Hôpital Bicêtre, AP-HP, Le Kremlin-Bicêtre, France.
Scand J Trauma Resusc Emerg Med. 2023 Jun 20;31(1):31. doi: 10.1186/s13049-023-01095-9.
Veno-arterial carbon dioxide tension difference (ΔPCO) and mixed venous oxygen saturation (SvO) have been shown to be markers of the adequacy between cardiac output and metabolic needs in critical care patients. However, they have hardly been assessed in trauma patients. We hypothesized that femoral ΔPCO (ΔPCO) and SvO (SvO) could predict the need for red blood cell (RBC) transfusion following severe trauma.
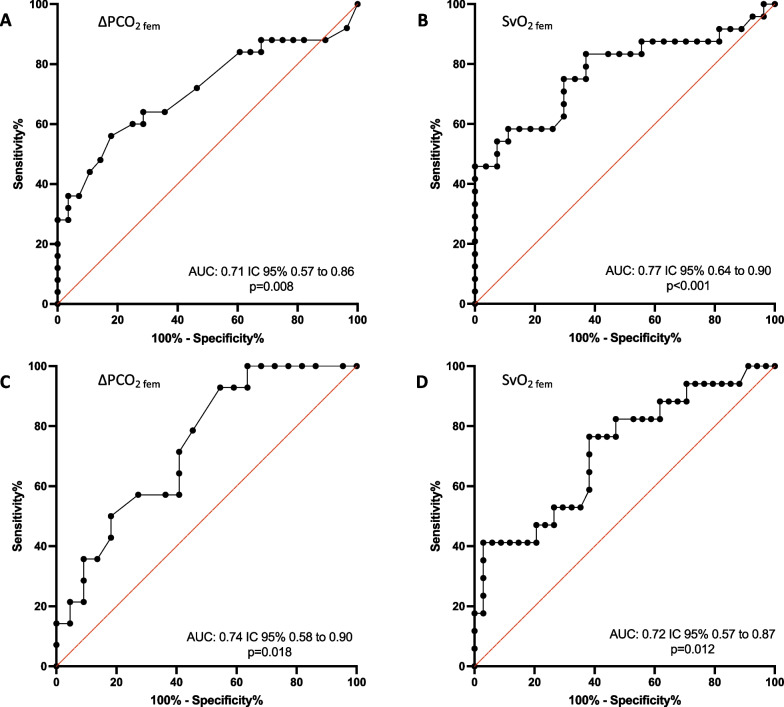
We conducted a prospective and observational study in a French level I trauma center. Patients admitted to the trauma room following severe trauma with an Injury Severity Score (ISS) > 15, who had arterial and venous femoral catheters inserted were included. ΔPCO SvO and arterial blood lactate were measured over the first 24 h of admission. Their abilities to predict the transfusion of at least one pack of RBC (pRBC) or hemostatic procedure during the first six hours of admission were assessed using receiver operating characteristics curve.
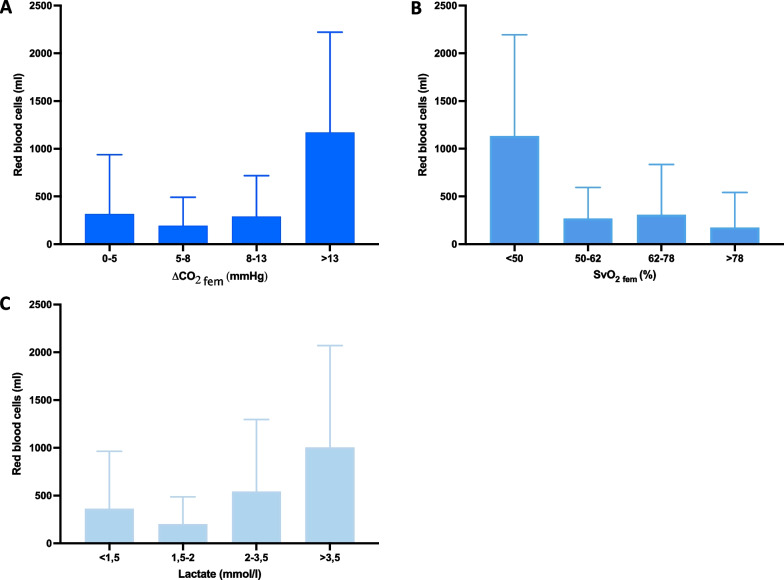
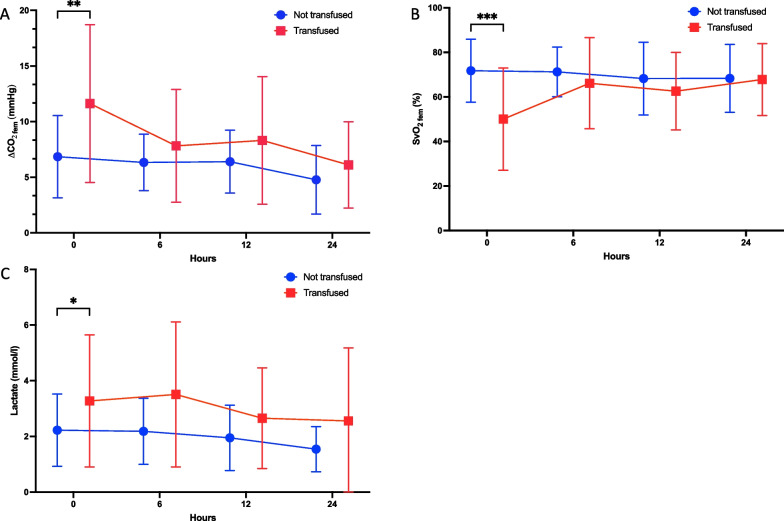
59 trauma patients were included in the study. Median ISS was 26 (22-32). 28 patients (47%) received at least one pRBC and 21 patients (35,6%) had a hemostatic procedure performed during the first six hours of admission. At admission, ΔPCO was 9.1 ± 6.0 mmHg, SvO 61.5 ± 21.6% and blood lactate was 2.7 ± 1.9 mmol/l. ΔPCO was significantly higher (11.6 ± 7.1 mmHg vs. 6.8 ± 3.7 mmHg, P = 0.003) and SvO was significantly lower (50 ± 23 mmHg vs. 71.8 ± 14.1 mmHg, P < 0.001) in patients who were transfused than in those who were not transfused. Best thresholds to predict pRBC were 8.1 mmHg for ΔPCO and 63% for SvO. Best thresholds to predict the need for a hemostatic procedure were 5.9 mmHg for ΔPCO and 63% for SvO. Blood lactate was not predictive of pRBC or the need for a hemostatic procedure.
In severe trauma patients, ΔPCO and SvO at admission were predictive for the need of RBC transfusion and hemostatic procedures during the first six hours of management while admission lactate was not. ΔPCO and SvO appear thus to be more sensitive to blood loss than blood lactate in trauma patients, which might be of importance to early assess the adequation of tissue blood flow with metabolic needs.
已证实,动静脉二氧化碳分压差(ΔPCO)和混合静脉血氧饱和度(SvO)是重症监护患者心输出量与代谢需求之间是否匹配的标志物。然而,它们在创伤患者中几乎没有被评估过。我们假设股动静脉二氧化碳分压差(ΔPCO)和 SvO(SvO)可预测严重创伤后红细胞(RBC)输血的需求。
我们在法国一级创伤中心进行了一项前瞻性、观察性研究。纳入因创伤严重且损伤严重程度评分(ISS)>15 分而被送入创伤室、且有股动脉和股静脉置管的患者。在入院的头 24 小时内,测量股动静脉 ΔPCO SvO 和动脉血乳酸。使用接收者操作特征曲线评估它们在入院最初 6 小时内预测至少输注 1 个单位 RBC(pRBC)或止血程序的能力。
59 例创伤患者纳入研究。ISS 中位数为 26(22-32)。28 例患者(47%)至少输注了 1 个 pRBC,21 例患者(35.6%)在入院最初 6 小时内进行了止血程序。入院时,ΔPCO 为 9.1±6.0mmHg,SvO 为 61.5±21.6%,血乳酸为 2.7±1.9mmol/L。与未输血的患者相比,输血的患者 ΔPCO 明显更高(11.6±7.1mmHg 比 6.8±3.7mmHg,P=0.003),SvO 明显更低(50±23mmHg 比 71.8±14.1mmHg,P<0.001)。预测 pRBC 的最佳阈值为 ΔPCO 为 8.1mmHg,SvO 为 63%。预测需要止血程序的最佳阈值为 ΔPCO 为 5.9mmHg,SvO 为 63%。血乳酸不能预测 pRBC 或需要止血程序。
在严重创伤患者中,入院时的 ΔPCO 和 SvO 可预测入院最初 6 小时内 RBC 输血和止血程序的需求,而入院时的乳酸则不能。与创伤患者的血乳酸相比,ΔPCO 和 SvO 似乎对失血更敏感,这可能对早期评估组织血流与代谢需求的匹配程度很重要。