Department of Internal Medicine, University Hospital Basel, Petersgraben 4, 4053 Basel, Switzerland.
Crit Care. 2010;14(6):R198. doi: 10.1186/cc9317. Epub 2010 Nov 3.
Acute respiratory failure (ARF) is responsible for about one-third of intensive care unit (ICU) admissions and is associated with adverse outcomes. Predictors of short- and long-term outcomes in unselected ICU-patients with ARF are ill-defined. The purpose of this analysis was to determine predictors of in-hospital and one-year mortality and assess the effects of oral beta-blockers in unselected ICU patients with ARF included in the BASEL-II-ICU study.
The BASEL II-ICU study was a prospective, multicenter, randomized, single-blinded, controlled trial of 314 (mean age 70 (62 to 79) years) ICU patients with ARF evaluating impact of a B-type natriuretic peptide- (BNP) guided management strategy on short-term outcomes.
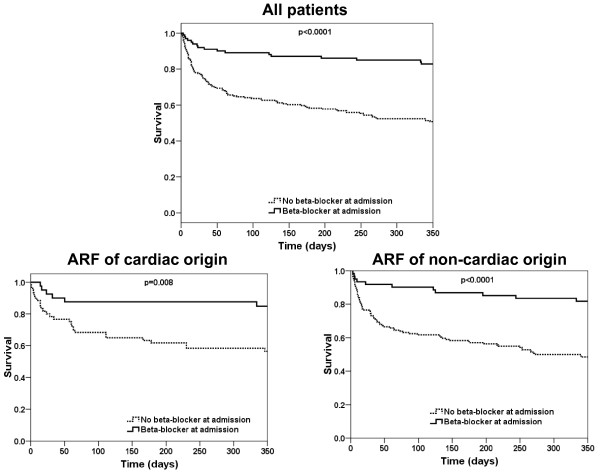
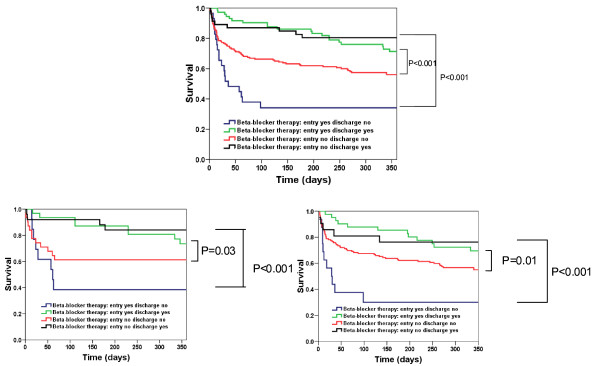
In-hospital mortality was 16% (51 patients) and one-year mortality 41% (128 patients). Multivariate analysis assessed that oral beta-blockers at admission were associated with a lower risk of both in-hospital (HR 0.33 (0.14 to 0.74) P = 0.007) and one-year mortality (HR 0.29 (0.16 to 0.51) P = 0.0003). Kaplan-Meier analysis confirmed the lower mortality in ARF patients when admitted with oral beta-blocker and further shows that the beneficial effect of oral beta-blockers at admission holds true in the two subgroups of patients with ARF related to cardiac or non-cardiac causes. Kaplan-Meier analysis also shows that administration of oral beta-blockers before hospital discharge gives striking additional beneficial effects on one-year mortality.
Established beta-blocker therapy appears to be associated with a reduced mortality in ICU patients with acute respiratory failure. Cessation of established therapy appears to be hazardous. Initiation of therapy prior to discharge appears to confer benefit. This finding was seen regardless of the cardiac or non-cardiac etiology of respiratory failure.
clinicalTrials.gov Identifier: NCT00130559.
急性呼吸衰竭(ARF)导致约三分之一的重症监护病房(ICU)入住,并与不良预后相关。未选择 ICU 患者 ARF 的短期和长期结局的预测因素尚未明确。本分析的目的是确定住院和一年死亡率的预测因素,并评估在纳入 BASEL-II-ICU 研究的 ARF 未选择的 ICU 患者中使用口服β受体阻滞剂的效果。
BASEL II-ICU 研究是一项前瞻性、多中心、随机、单盲、对照试验,纳入 314 名(平均年龄 70(62 至 79)岁)ARF 的 ICU 患者,评估 B 型利钠肽(BNP)指导管理策略对短期结局的影响。
住院死亡率为 16%(51 例),一年死亡率为 41%(128 例)。多变量分析评估入院时口服β受体阻滞剂与住院(HR 0.33(0.14 至 0.74),P = 0.007)和一年死亡率(HR 0.29(0.16 至 0.51),P = 0.0003)的风险降低相关。Kaplan-Meier 分析证实,入院时服用口服β受体阻滞剂的 ARF 患者死亡率较低,并且进一步表明,在与心脏或非心脏原因相关的 ARF 患者的两个亚组中,入院时口服β受体阻滞剂的有益效果是真实的。Kaplan-Meier 分析还表明,在出院前给予口服β受体阻滞剂可显著降低一年死亡率。
已确立的β受体阻滞剂治疗似乎与 ICU 急性呼吸衰竭患者的死亡率降低相关。停止既定治疗似乎有危险。在出院前开始治疗似乎有益。无论呼吸衰竭的心脏或非心脏病因如何,都可以看到这种发现。
clinicalTrials.gov 标识符:NCT00130559。