Dept of Surgery North Shore Univ. Hosp. Division of Surgical Oncology, Manhasset NY, USA; Med. Univ of South Carolina and Neogenix Oncology Inc. Great Neck NY, USA.
J Cancer. 2010 Nov 3;1:209-22. doi: 10.7150/jca.1.209.
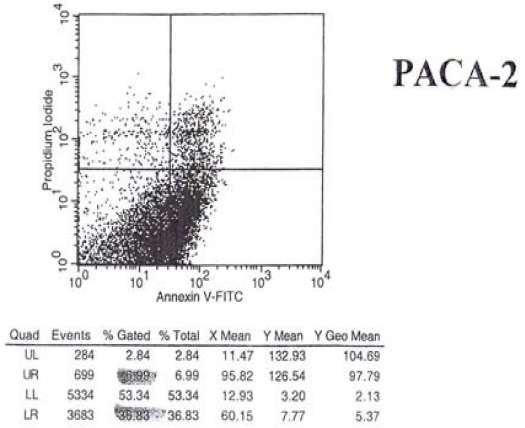
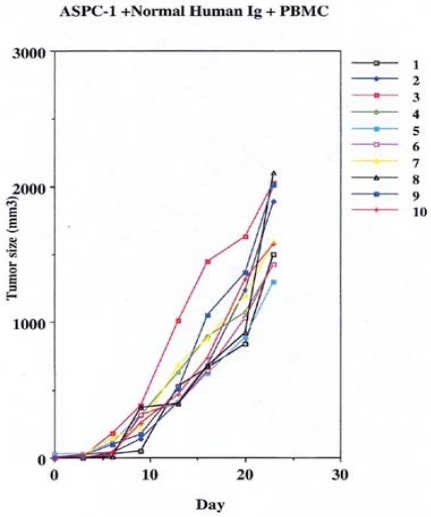
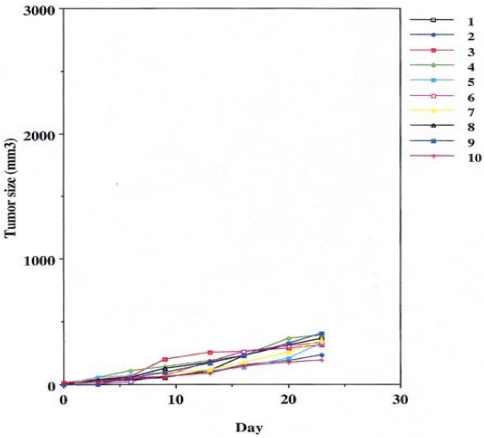
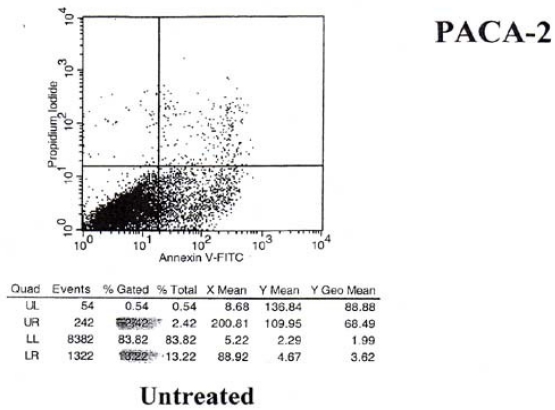
Monoclonal antibodies developed against immunogenic proteins (Tumor Specific Antigens/TSA's) that are expressed in human cancers, display a unique behavioral pattern. They appear to serve in a dual role. This includes the early recognition of these immunogenic membrane proteins that can serve as diagnostic markers, and the targeting of such markers for the destruction of the tumor, primarily thru ADCC.The monoclonals (mAbs) that we have developed against specific immunogenic tumor membrane proteins have been studied in detail. These tumor proteins, when first defined, were referred to as tumor associated antigens. With the ability of the mAbs to demonstrate therapeutic antitumor activity in those patients with relatively advanced malignancies, the term tumor specific was introduced. Monoclonals that we were able to develop from tumor specific proteins derived from colon and pancreas cancer were found capable of targeting those tumors to induce apoptosis. We were also able to define immunogenic membrane proteins from lung (squamous and adenoCa) as well as prostate neoplasms. Monoclonals developed from these tumor antigens are in the initial phases of investigation with regard to their specificity and antitumor activity.Mabs capable of targeting the malignancies noted above were produced following immunization of BALBc mice with the Tumor Specific Antigens. The hybridomas that were screened and found to express the antibodies of interest appeared for the most part as IgG2a's. It became apparent after a short period of time that stability of the Fab CDR loops as well as the therapeutic efficacy of the hybridoma mAbs could be lost. Stability was achieved by chimerization and or humanization. The resulting mAbs were found to switch their isotypes to an IgG1 subsequent to chimerization and or humanization, when expressed in CHO cells. The monoclonals, so produced, were not only more efficient in controlling tumor growth but minimized the development of a HAMA response.Because of 1) the specificity of this group of monoclonal antibodies in targeting well defined immunogenic proteins that were expressed on the tumor cell membrane,2) their lack of cross reactivity to normal tissue, 3) relatively low toxicity when delivered intravenously, 4) rapid targeting of tumor cell populations (4-6 hrs in vitro) and their 5) ability to destroy xenograft transplants (in vivo) within days of delivery, these mAbs were felt to be ideal for possible use in the treatment of patients with recurrent and or metastatic tumors.Initial clinical studies have been planned for following the filing of an IND. It is required by FDA that the potential effects of tumor control and toxicity be defined using the naked antibodies produced under GMP conditions, In those situations where patients with recurrent malignancies are to be studied we have come to realize that a number of factors can influence the response to monoclonal therapy. This includes the amount of shed antigen in the serum at the time of treatment that could initiate immune complex formation as well as the shedding of inhibitory material into the serum possibly effecting an immune response. As such we plan to eventually employ the therapeutic mAbs in combination with chemotherapy as a means of enhancing the immunogenicity of the tumor system being treated and to possibly weaken the malignant growth for easier destruction by the mAb. We will also look at the combination of mAbs with immunostimulants such as GMCSF and IL-2 (fusion proteins) and eventual conjugation of the mAbs with alpha and possibly B-emitters to help in targeting bystander cells. The present paper reviews the potential therapeutic value of such mAbs in the treatment of recurrent malignancies, especially those having failed chemotherapy in established clinical trials.
针对在人类癌症中表达的免疫原性蛋白(肿瘤特异性抗原/TSA)开发的单克隆抗体表现出独特的行为模式。它们似乎具有双重作用。这包括早期识别这些可作为诊断标志物的免疫原性膜蛋白,并针对这些标志物进行靶向治疗以破坏肿瘤,主要通过 ADCC。我们针对特定的免疫原性肿瘤膜蛋白开发的单克隆抗体已经进行了详细研究。这些肿瘤蛋白最初被定义为肿瘤相关抗原。由于单克隆抗体能够在那些患有相对晚期恶性肿瘤的患者中显示出治疗性抗肿瘤活性,因此引入了肿瘤特异性这个术语。我们能够从源自结肠癌和胰腺癌的肿瘤特异性蛋白中开发出的单克隆抗体能够靶向这些肿瘤以诱导细胞凋亡。我们还能够从肺癌(鳞状细胞癌和腺癌)以及前列腺肿瘤中定义免疫原性膜蛋白。从这些肿瘤抗原开发的单克隆抗体正处于研究其特异性和抗肿瘤活性的初始阶段。在 BALBc 小鼠中用肿瘤特异性抗原免疫后,产生了能够靶向上述恶性肿瘤的单克隆抗体。筛选出并发现表达感兴趣抗体的杂交瘤在大多数情况下表现为 IgG2a。在很短的时间内就发现,Fab CDR 环的稳定性以及杂交瘤单克隆抗体的治疗效果可能会丢失。通过嵌合化和/或人源化实现了稳定性。当在 CHO 细胞中表达时,发现产生的单克隆抗体将其同种型转换为 IgG1。如此产生的单克隆抗体不仅在控制肿瘤生长方面更有效,而且还最大程度地减少了 HAMA 反应的发展。由于 1)该组单克隆抗体在靶向肿瘤细胞膜上表达的定义明确的免疫原性蛋白方面的特异性,2)它们与正常组织无交叉反应性,3)静脉内给药时相对较低的毒性,4)快速靶向肿瘤细胞群(体外 4-6 小时)以及 5)能够在几天内破坏异种移植移植物(体内),因此这些单克隆抗体被认为非常适合可能用于治疗复发性和/或转移性肿瘤的患者。在提交 IND 后,已计划进行初步临床研究。FDA 要求使用在 GMP 条件下生产的裸抗体来定义肿瘤控制和毒性的潜在影响。在研究复发性恶性肿瘤的患者时,我们已经意识到许多因素会影响单克隆治疗的反应。这包括在治疗时血清中脱落抗原的量,这可能引发免疫复合物的形成,以及可能影响免疫反应的抑制性物质的脱落。因此,我们计划最终将治疗性单克隆抗体与化疗联合使用,作为增强正在治疗的肿瘤系统的免疫原性并可能削弱恶性生长以便更容易被单克隆抗体破坏的手段。我们还将研究单克隆抗体与免疫刺激剂(如 GMCSF 和 IL-2(融合蛋白))的组合,并最终将单克隆抗体与α和可能的β发射器结合,以帮助旁观者细胞的靶向。本文综述了此类单克隆抗体在复发性恶性肿瘤治疗中的潜在治疗价值,特别是在已建立的临床试验中化疗失败的肿瘤。